 Close
Close

So why is a GP publishing about Covid radiology?
By Nathan Davies, on 31 July 2020
By Melvyn Jones
I have just co authored a BMJ piece on chest radiographs with Covid pneumonia – The role of chest radiography in confirming covid-19 pneumonia So why is a GP publishing about Covid radiology? 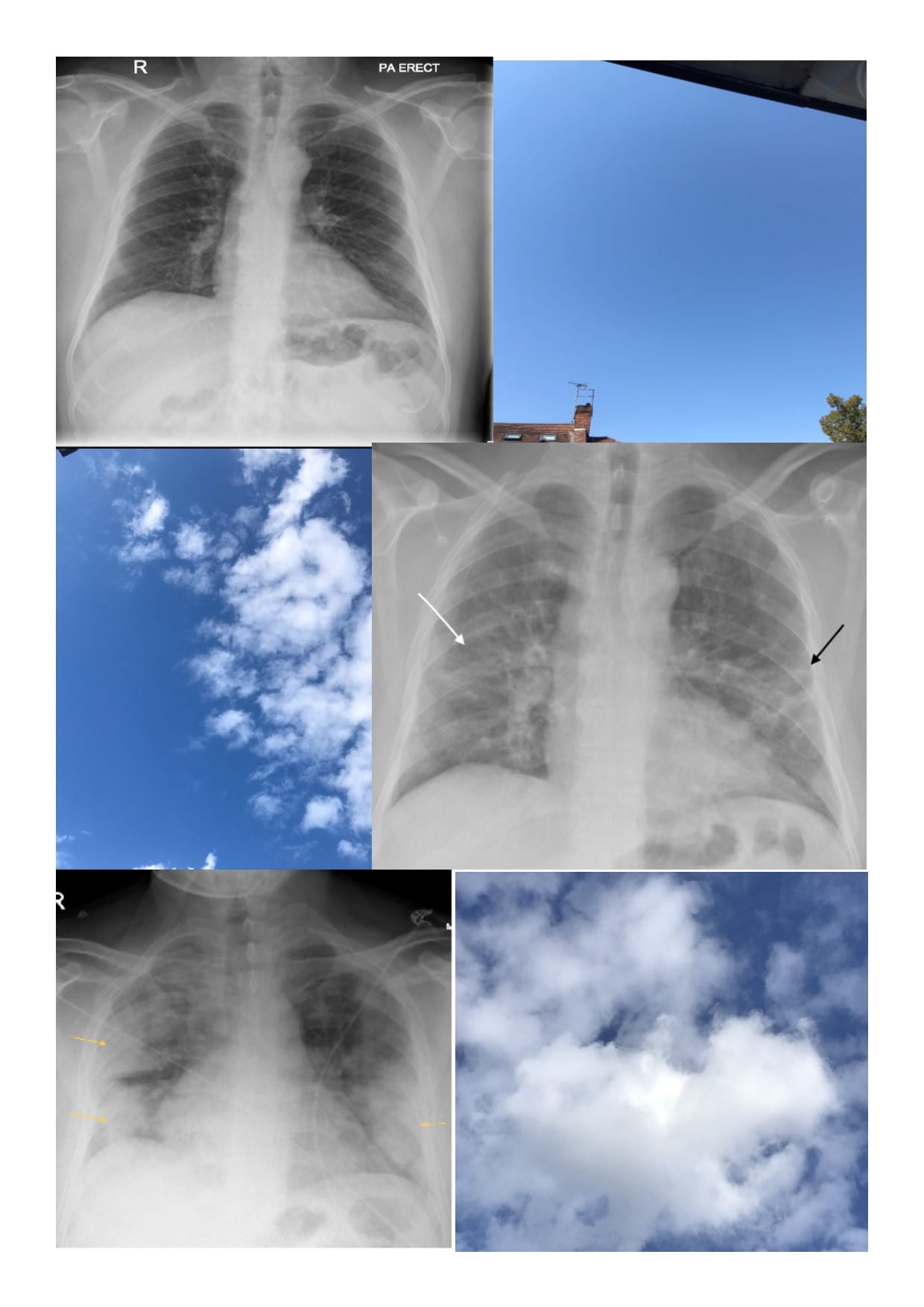
My wife is a radiologist with a special interest in chest radiology and a love of a good chest x-ray; back in March she was starting to see the x-rays of the first patients with covid pneumonia and she was shocked. She hadn’t ever seen x-rays like this. This was something really different.
There were real fears that hospitals would be overwhelmed and we knew clinicians who never normally look at a chest x-ray anymore were being marshalled in to support the covid response. Would they know what to look for on the chest x-ray? Could we do something to help? So I wrote to the BMJ pitching an idea on the 22nd March. They liked the idea and commissioned us to do a “Practice pointer”, not a traditional systematic review but an article based on evidence and clinical experience. I interviewed my wife to capture the key points and while she was on call went searching for good images. My literature search revealed 20 articles and only 1 related to Chest x-rays, there really wasn’t much out there. We had our submission ready and posted it on the 30th March and by that stage 1200 UK patients had died of Covid.
I needed to understand a bit of radiology to work though the literature. What is ground glass opacification (“the lung markings are still visible through the Covid changes”) and how it is different to consolidation- key concepts with Covid pneumonia. Covid lockdown meant the possibility of eating breakfast outside and thinking things through in a slightly less pressured environment. Should I admit to looking at the cloud formations during those few weeks of glorious weather? I did, I do. Cirrus clouds were my ground glass, I could still see the sky through these light feathery clouds, cumulonimbus was my consolidation; thick, opaque and ominous.
There then followed 6 revisions and further major changes requested by the team that ready it for publication. It went out to 7 different peer reviewers; many of whom made valuable but conflicting requests for changes but the overwhelming message was – this needs to be out there, now. We also needed input from a physician who was in the thick of it- how were they actually using imaging as part of their assessments of breathless Covid patient? I was working with James Piper – an Acute Medicine doctor at the Royal Free as part of the MB BS teaching programme and he was happy to help.
We turned round each iteration within 48-72 hours but still the requests for changes came. The numbers of UK deaths went relentlessly up. Eventually it was accepted, type set and finally published on the 16th July. UK deaths had now exceeded 45,000, Google scholar had hundreds of Covid articles and we were coming out of lockdown. It was a pleasure to see it finally published but there was a real sense that it was just too late. That’s the thing with the BMJ though; the day it was published it was downloaded over a 1000 times, two weeks later it has been viewed over 7000 times. The really helpful thing though for someone who is not a big user of social media, was seeing who Tweeted about it and where. The BMJ link had been re-tweeted 147 times and to places like South Africa, South America and India- all parts of the world which were now facing their 1st waves of this terrible disease and today the newspaper headline is “Europe faces its 2nd peak”. It may be of use to a clinician somewhere having to manage yet another patient with this awful disease, so may be we could and did do something?