Across the globe, people are living longer. Many countries – including the UK – have responded by raising the age of retirement. By 2028, UK citizens will need to be 67 years old to receive their state pension, and further increases have been recommended by both government and independent reviews.
But there’s one major issue with this: most employees in the UK already stop working before the current state pension age of 65. For some, early retirement can be a positive life change which means they can afford to stop working. But for others, early retirement is a result of poor health or unemployment, which can eat into savings and widen inequalities among older people.
Previous studies have shown that in areas where there are more unemployed people, older people are also more likely to leave the workforce. In the past, researchers thought this was because older workers are more likely to be made redundant and have a harder time finding another job when they are unemployed.
But our new research shows that the link between local unemployment and retirement age actually depends on where people live as young adults. Specifically, people in their 20s who live in areas where there are fewer jobs are more likely to be unemployed and in poor health at mid-life – and these are two significant causes of early retirement.
There were 2,526 cohort members, who told us whether they had retired from their main occupation or were still in work. First, we explored where they had lived in childhood (at age four), young adulthood (age 26) and mid-life (age 53). Then, for all three ages, we looked at census data to find out how many working-age people in their local authority were unemployed at the time.
By the age of 68, more than 80% of the people in the cohort had retired, with the average age of retirement being around 59 years. As seen in previous studies, those who lived in areas with higher levels of unemployment at mid-life, also tended to retire earlier. For each 5% increase in local unemployment, people retired on average roughly 1.5 years earlier.
Long-term effects
But when we started to delve into where cohort members had lived earlier in their lives – as well as considering their health, employment and education history – we realised just how strongly unemployment levels in the local area during early adulthood continued to affect people throughout their lives.
If a cohort member lived in a local authority where there was more unemployment than average as a child, it was also likely that they would live somewhere similar as an adult. And those who lived in areas with higher than average unemployment rates as young adults then went on to have poorer health and were more likely to be unemployed at mid-life – compared with those who lived in areas with lower unemployment rates.
Researchers have found that health and employment status strongly predict what age people retire. We found this as well, with cohort members who were unemployed at mid-life retiring on average about five years earlier than those who were working full time at the same age.
What’s more, we found that the link between where people live in their mid-life and their retirement age can actually be traced right back to where they lived in their 20s. So the experiences people had when they were younger had a long term impact on their health and employment status at mid-life.
For example, someone who had moved in their early 20s to Guildford, where there was high employment, was more likely to still be in work when they reached mid-life, than someone who had lived in their 20s in Glasgow – where unemployment was high – regardless of where either lived later in life (although it is likely both will have lived in the same or equivalent employment area in their 50s).
Our findings imply that people should think carefully about how where they live might affect their career. People seem to know that it’s easier to get a job in areas where there are more jobs available – indeed, graduates tend to migrate into urban centres with more employment opportunities. Our research shows that these early career decisions can have consequences into people’s retirement years.
If the government wants to encourage people to stay in work longer, it should give older workers the support they need to stay in work and in good health. It could also help them maintain their employment, even when they’re not in the best of health – for example by adapting workplaces for older workers, or encouraging flexible working. By improving job opportunities for young people living in places with high unemployment, it could help people to keep working for
Where you live in your 20s affects when you retire – here’s how
Where you decide to live will impact your career. Shutterstock.
Across the globe, people are living longer. Many countries – including the UK – have responded by raising the age of retirement. By 2028, UK citizens will need to be 67 years old to receive their state pension, and further increases have been recommended by both government and independent reviews.
But there’s one major issue with this: most employees in the UK already stop working before the current state pension age of 65. For some, early retirement can be a positive life change which means they can afford to stop working. But for others, early retirement is a result of poor health or unemployment, which can eat into savings and widen inequalities among older people.
Previous studies have shown that in areas where there are more unemployed people, older people are also more likely to leave the workforce. In the past, researchers thought this was because older workers are more likely to be made redundant and have a harder time finding another job when they are unemployed.
But our new research shows that the link between local unemployment and retirement age actually depends on where people live as young adults. Specifically, people in their 20s who live in areas where there are fewer jobs are more likely to be unemployed and in poor health at mid-life – and these are two significant causes of early retirement.
There were 2,526 cohort members, who told us whether they had retired from their main occupation or were still in work. First, we explored where they had lived in childhood (at age four), young adulthood (age 26) and mid-life (age 53). Then, for all three ages, we looked at census data to find out how many working-age people in their local authority were unemployed at the time.
By the age of 68, more than 80% of the people in the cohort had retired, with the average age of retirement being around 59 years. As seen in previous studies, those who lived in areas with higher levels of unemployment at mid-life, also tended to retire earlier. For each 5% increase in local unemployment, people retired on average roughly 1.5 years earlier.
Long-term effects
But when we started to delve into where cohort members had lived earlier in their lives – as well as considering their health, employment and education history – we realised just how strongly unemployment levels in the local area during early adulthood continued to affect people throughout their lives.
If a cohort member lived in a local authority where there was more unemployment than average as a child, it was also likely that they would live somewhere similar as an adult. And those who lived in areas with higher than average unemployment rates as young adults then went on to have poorer health and were more likely to be unemployed at mid-life – compared with those who lived in areas with lower unemployment rates.
Researchers have found that health and employment status strongly predict what age people retire. We found this as well, with cohort members who were unemployed at mid-life retiring on average about five years earlier than those who were working full time at the same age.
What’s more, we found that the link between where people live in their mid-life and their retirement age can actually be traced right back to where they lived in their 20s. So the experiences people had when they were younger had a long term impact on their health and employment status at mid-life.
For example, someone who had moved in their early 20s to Guildford, where there was high employment, was more likely to still be in work when they reached mid-life, than someone who had lived in their 20s in Glasgow – where unemployment was high – regardless of where either lived later in life (although it is likely both will have lived in the same or equivalent employment area in their 50s).
Our findings imply that people should think carefully about how where they live might affect their career. People seem to know that it’s easier to get a job in areas where there are more jobs available – indeed, graduates tend to migrate into urban centres with more employment opportunities. Our research shows that these early career decisions can have consequences into people’s retirement years.
If the government wants to encourage people to stay in work longer, it should give older workers the support they need to stay in work and in good health. It could also help them maintain their employment, even when they’re not in the best of health – for example by adapting workplaces for older workers, or encouraging flexible working. By improving job opportunities for young people living in places with high unemployment, it could help people to keep working for longer.
Emily Murray, Senior Research Fellow, Department of Epidemiology & Public Health, UCL
The rise of globalisation and the 24/7 economy are fuelling demands for people to work long hours and weekends. But what’s the evidence about how these ways of working link with depression? Gill Weston and colleagues from the International Centre for Lifecourse Studies in Society and Health at UCL and Queen Mary University of London found such working conditions are linked to poorer mental health in women.
Across the globe, the effects of overwork are becoming apparent. In eastern Asian countries the risk of death due to overwork has increased. In the UK, work-related stress accounts for millions of lost working days every year.
Within the EU, a significant proportion of people have to work unsociable hours – with nearly a quarter working most Saturdays and a third working at least one Sunday a month. But despite this, there isn’t much clear evidence about the links between work patterns and mental health.
Some studies have found a connection between unsociable work patterns and depression. But many of the studies only focused on men, some only looked at specific types of worker or workplaces and few took account of work conditions such as whether workers had any control over how fast they worked.
To address these gaps, we set out to look for links between long or irregular hours and depression using a large nationally representative sample of working men and women in the UK. We particularly wanted to look at whether there were differences between men and women because research has shown that work is organised, experienced and rewarded differently for men and women, and because men and women react differently to overwork and time pressure.
We used data from Understanding Society, which surveys people living in 40,000 households across the UK. In particular we focused on information about working hours, weekend working and working conditions collected from 11,215 working men and 12,188 working women between 2010 and 2012. They had completed a questionnaire designed to study levels of psychological distress.
Who works the most?
We found men tended to work longer hours in paid work than women, and having children affected men’s and women’s work patterns in different ways: while mothers tended to work fewer hours than women without children, fathers tended to work more hours than men without children.
Two thirds of all men worked weekends, compared with half of all women. Those who worked all or most weekends were more likely to be in low skilled work and to be less satisfied with their job and their earnings than those who only worked Monday to Friday or some weekends
Which workers have the most depressive symptoms?
Women, in general, are more likely to be depressed than men, and this was no different in our study.
Independent of their working patterns, we also found that workers with the most depressive symptoms were older, smokers, on lower incomes, in physically demanding jobs, and who were dissatisfied at work.
Arelong and irregular hourslinked to depression?
Taking these findings and other factors into account, when we looked at the mental health effects of work patterns on men and on women, the results were striking: while there was little or no difference in depressive symptoms between men who worked long hours and those who did not, this was not the case for women.
Those women who worked 55 hours or more per week had a higher risk of depression than women working a standard 35-40 hour week.
Similarly, weekend working showed differences for men and women. Compared to workers who only worked on weekdays, men who worked weekends also had a greater number of depressive symptoms, but only if they had little control at work or were dissatisfied with work. Whereas for women, regardless of their control or satisfaction, working most or all weekends was linked to more depressive symptoms.
Why might women suffer more than men while working these antisocial hours?
There might be a number of reasons why women might be more affected than men:
Women who work long hours are in a minority – just four per cent of them in our sample worked 55 hours or more per week. This may place them under additional pressure.
Women working longer hours tend to be in male-dominated occupations, and this may also contribute to stress.
Women working weekends tend to be concentrated in low-paid service sector jobs, which have been linked to higher levels of depression.
Many women face the additional burden of doing a larger share of domestic labour than men, leading to extensive total work hours, added time pressures or overwhelming responsibilities.
What should be done about these risks?
Our findings should encourage employers and policy-makers to think about how to reduce the burdens and increase support for women who work long or irregular hours – without restricting their ability to work when they wish to. More sympathetic working practices could bring benefits both for workers and for employers – of both sexes.
Since their arrival in the UK in 2010/11, electronic cigarettes (e-cigarettes or vapes) have rapidly become the most popular aid to help people quit smoking. With evidence continuing to grow showing that vaping 1) poses a small fraction of the risks of smoking and 2) improves smoking quit success, Public Health England have restated that smokers who are struggling to quit should ‘try switching to an e-cigarette’ along with seeking help by trained specialists. But what does this mean for existing inequalities in smoking?
Following a steady decline over the past decade, 15% of the population in England are estimated to currently smoke. However, smoking rates fall along a social gradient, with one in four people from disadvantaged socio-economic groups smoking, compared with one in ten from more affluent groups. This means that a disproportionate number of the ~78,000 deaths and the ~485,000 hospital admissions caused by smoking in England each year fall upon the disadvantaged.
Given their popularity (used by >30% of smokers making a quit attempt) and generally lower cost compared with cigarettes, e-cigarettes have potential to help reduce inequalities in smoking cessation. However, a concern during the early period in which e-cigarettes first arrived on the UK market was that they were more popular with better off smokers. If the devices boost quit success, which appears to be the case, then these differences in use across the social gradient could potentially lead to disadvantaged smokers being left behind, thus worsening the existing inequalities.
Keeping up with change
Since their creation in 2003 by a Chinese pharmacist Hon Lik, e-cigarettes have continued to evolve with novel designs and more effective nicotine delivery systems being rolled out each year. The Smoking Toolkit Study (STS), set up by the Tobacco and Alcohol Research Group at UCL to monitor population trends in smoking in England, is one way that researchers and policy makers can keep up with this ever-changing landscape of e-cigarette use and assess whether they promote or detract from reducing smoking rates.
Using STS data from 2014 to 2017, our recent research published in the journal Addiction was the first of kind to look at the use of e-cigarettes by different socio-economic groups at the population level. Our study analysed data from over 81,000 adults in England, including 16,000 past-year smokers, 5,300 smokers making a quit attempt and 13,500 long-term ex-smokers. E-cigarette use in each group was assessed using participant social grade (based on occupation) or housing status as key indicators of socio-economic position.
Narrowing differences among smokers
Our analysis indicated that in the three years from 2014 to 2016, disadvantaged smokers were around half as likely to use e-cigarettes. However, by 2017 this difference was no longer evident. Similarly, there were no differences in e-cigarette use by smokers making a quit attempt. Should this absence of difference between socioeconomic groups remain going forward then it is unlikely that the use of e-cigarettes among smokers and quit attempters will have a persistent impact on inequalities. However, it will be important to investigate whether there are socio-economic differences in the success of quit attempts with e-cigarettes, something which researchers in our group have been looking into.
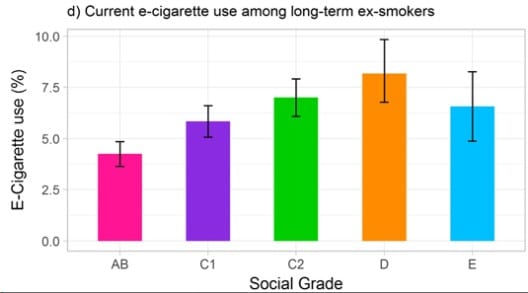
Greater e-cigarette use among disadvantaged ex-smokers
Our research also showed a different pattern among smokers who had been quit for over a year, with disadvantaged ex-smokers more than twice as likely to use an e-cigarette. This could have important implications, and really depends on whether e-cigarettes prevent ex-smokers from relapsing back into smoking tobacco. If that were true (unfortunately there isn’t much research on this yet) then e-cigarette use would protect more disadvantaged smokers from slipping back into smoking and act to reduce inequalities; an equity-positive effect.
The wider picture
Inequalities in smoking are driven by a complex and nuanced system acting at the population, community and individual level. Reducing disparity requires action at all levels such as tobacco taxes, public health media and education campaigns and individual specialist support that targets the neurobiological and motivational components of nicotine addiction that dependent smokers struggle with. E-cigarettes are not a magic wand for quitting smoking. Rather, given their popularity and similar effectiveness to other forms of nicotine replacement therapy, they are part of a toolbox of interventions that are contributing to the continuing decline in smoking in the UK. If they are available, affordable and able to deliver nicotine effectively without the loss of social identity that some smokers subscribe to, e-cigarettes may also help redress the persistent inequalities in smoking.
Loren Kock (@loren_kock.) is a Cancer Research UK funded PhD student in Epidemiology and Public health, working within the UCL Tobacco and Alcohol Research Group. His research focusses on how e-cigarettes and other smoking cessation interventions impact on socio-economic inequalities in smoking cessation.
A new mobile phone will be in the pockets of many teenagers as they head back to school in the coming days. The period between Xmas and New Year will have been spent signing up for social media apps where they can chat, share photos and videos with friends, all part of the excitement of owning a new device. But how many of these young people and their parents are aware of the potential pitfalls of spending too much time on social media sites? And what can parents, teachers and young people themselves do to maximize the benefits of life online whilst minimising those pitfalls? It’s a question that Yvonne Kelly, Director of the ESRC International Centre for Life course Studies at UCL and colleagues have been asking as part of a major programme of research on social media use and young people’s wellbeing.
Today they publish key new research, which provides much-needed new evidence on the links between heavy social media use and depression in teenagers. The research shines light on the underlying processes that could be at work and that might explain the link between the two. Here, Yvonne explains how their research might help policymakers, educators, parents and young people themselves better understand and prevent the potential pitfalls of living too much of their life on social media platforms.
2018 has seen a growing chorus of voices including those of the former and current Health Secretaries, Jeremy Hunt and Matt Hancock calling for a thorough investigation of the links between social media use and the growing numbers of young people struggling with mental health issues. Indeed Matt Hancock issued “an urgent warning” on the potential dangers of social media on children’s mental health, stating that the threat of social media on mental health is similar to that of sugar on physical health.
The Chief Medical Officer, Dame Sally Davies has been tasked by the Government with leading that investigation and with coming up with evidence based recommendations around what constitutes safe social media use and what changes need to be made and by whom to make that a reality. The Royal College of Paediatrics and Child Health (RCPCH) recently issued the first ever guidance on managing children’s screen time, calling for further research particularly into social media.
In recent months, we and others have submitted written and oral evidence to two Parliamentary inquiries in this area and had discussions with the Royal Society for Public Health which is campaigning actively to get us all thinking harder about our social media use.
We’ve talked about our early research showing that 10 year-old girls who used social media sites for chatting had more social and emotional problems at age 15 than their peers who used them less or not at all. Those problems continued to get worse as they got older.
Our new research published in The Lancet’s EClinical Medicine draws stronger links between heavy social media use and depressive symptoms in girls and boys at the age of 14. We look at the possible ways in which social media use might linked to depressive symptoms. We consider 4 potential pathways – through young people’s sleep patterns, their experiences of online harassment, body image and self-esteem. It is the first research to look at all of these potential pathways at the same time.
Our data for this research came from the Millennium Cohort Study, which has followed the lives of some 19,000 children born at the turn of the century. This piece of research, looked at the social media use and mental health of nearly 11,000 of the study’s participants.
Social media use
In line with our earlier research, we saw that girls were heavier users of social media than boys with two fifths of them using it for more than 3 hours per day (compared with one fifth of boys). Girls were a lot less likely NOT to use social media at all (4 per cent girls and 10 per cent boys).
Examining the underlying processes that might be linked with social media use and depression, we saw a number of really striking findings including:
40 per cent of girls and 25 per cent of boys had experience of online harassment or cyberbullying
78 per cent of girls and 68 per cent of boys were unhappy with their body/weight and 15 percent girls and 12 per cent of boys were unhappy with their appearance
13 per cent of girls and 9 per cent of boys had low self-esteem
13 per cent of girls and 11 per cent of boys reported getting fewer than 7 hours sleep per night and 40 per cent of girls and 28 per cent of boys said their sleep was often disrupted
Girls, it seems from these findings, are struggling more with these aspects of their lives than boys – in some cases considerably more. When we turned our attention to the signs of depression exhibited by our participants, we could see that here too girls fared worse with scores on average twice as high as those of boys.
The link between social media use and depressive symptoms was stronger for girls compared with boys. For girls, greater daily hours of social media use corresponded to a stepwise increase in depressive symptoms and the percent with clinically relevant symptoms. For boys, higher depressive symptom scores were seen among those reporting 3 or more hours of daily social media use.
There was a clear link between social media use and all the pathways we investigated – more time spent on social media related to having poorer sleep, more experiences of on-line harassment, unhappiness with the way they look and low self esteem. In turn, these things were directly related to having depressive symptoms.
A closer look at the pathways was also revealing. The most important routes from social media use to depressive symptoms were shown to be via poor sleep and online harassment.
Social media use linked directly to having poor sleep which in turn was related directly to having more depressive symptoms. The role of online harassment was more complex, with multiple pathways through poor sleep, self-esteem and body image, all of which linked directly to depressive symptoms.
Potential pitfalls and key routes
Our findings add weight to the growing evidence base on the potential pitfalls associated with lengthy time spent engaging on social media. In particular they point to poor sleep and online harrassment as being key routes between social media use and depression.
These findings are highly relevant to current policy development on guidelines for the safe use of social media and calls on industry to more tightly regulate hours of social media use for young people. They add weight to the Screen Time Guidance issued by the RCPCH today, particularly the suggestion to set and agree child appropriate time limits on screen use.
When it comes to social media use specifically, our research indicates that the a similar approach could be useful. Clinical, educational and family settings are all potential points of contact where young people could be encouraged and supported to reflect not only on their social media use, but also other aspects of their lives including on-line experiences and their sleep patterns.
At home, families may want to reflect on when and where it’s ok to be on social media and agree limits for time spent online. Curfews for use and the overnight removal of mobile devices from bedrooms might also be something to consider. School seems an obvious setting for children and young people to learn how to navigate online life appropriately and safely and for interventions aimed at promoting self-esteem. Clearly a large proportion of young people experience dissatisfaction with the way they look and how they feel about their bodies and perhaps a broader societal shift away from the perpetuation of what are often highly distorted images of idealised beauty could help shift these types of negative perceptions.
As we head into 2019, millions of young people will be getting their first experiences of life online using the devices they got for Xmas. They will rapidly become expert at downloading apps, posting photos and interacting with their peers. With the gift there was no instruction manual to help them understand and navigate some of the pitfalls our research outlines. We hope our work brings, at least, some guidance for all those keen to ensure these children continue to thrive and do well, so that they enjoy the benefits that new digital technology brings whilst staying safe and happy.
The 13th of December 2017 dawned like any other day. I was sitting at my desk with my favourite coffee preparing to dive into another day of researching…when a Twitter notification popped up:
Professor Jenny Head, my supervisor and head of our research group at the time, had provided a link to a video recording of the all parliamentary meeting of the Women’s & Equality sub-committee. I clicked over & started to listen. Fifteen minutes into the recording, something wonderful happened:
Someone mentioned my research. My research. MY. RESEARCH. In a parliamentary meeting.
To put it mildly, I was elated.
Isn’t this what we as researchers aspire to in our work? That the findings of our work makes its way into the ears of the people who make the decisions? That someday, hopefully, what we have researched will change policy, improve health & well-being of the population and generally improve the lives of all our brethren?
But I get ahead of myself.
I don’t know whether my findings being relayed in a parliamentary meeting has changed anything (yet). What I do know is that it didn’t happen by accident. It wasn’t entirely planned either, but a series of steps and activities that our project, RenEWL (Research on Extending Working Lives), undertook made the outcome much more likely. I share them with you now so that you will hopefully be even more successful than I was.
Emily’s top tips for getting your research mentioned in Parliament:
Start Early – at RenEWL, we set up an impact sub-group from day one. We charted out ideas for impact events, discussed who we wanted to target with our research and mapped out timelines. This is important. If we had waited until we had had actual research results, we wouldn’t have had the time to plan effective events.
*Note: If you are not a part of a large group, or solo researching, find an impact officer at your institution. If you don’t have one of those, find a researcher you admire for their impact work and ask them how they plan out their impact.
Build Relationships – One of our first impact events was a launch event we held within the first 6 months of our project. We invited a select group of experts in government, academic and the third-sector who we knew worked in our subject area. Part of the event was to introduce the project and project plans to the participants. But what I also think was particularly important, was to build in time to listen to THEM. We set up group discussions where we asked what they thought of our project aims, but also importantly what topic areas they were interested in that we were missing.
Bring in the experts – One of the initial collaborators on our programme was the International Longevity Centre (ILC-UK). ILC-UK has vast experience with planning events and disseminating results to policy-makers. Our project commissioned them to help disseminate our findings to policy-makers. I believe it was this collaboration which was instrumental in making our policy maker-focused event ‘Overcoming Inequalities: Addressing barriers to extending working lives’ such a success. They additionally briefed individual ministers, government units and journalists.
Stay Aware – Find our how Parliament works. To get started, there are simple guides on the Parliament’s website. Here is the guide for Select Committees. Sign up for the UK parliament newsletter to receive notifications of events and offered trainings. Find out what topic areas are accepting submissions of evidence here. We submitted evidence to a number of government consultations, including in person to the Independent Review of the State Pension Age.
Act quickly – Or at least be prepared to act quickly. Don’t wait for a consultation to pop up on your radar to start drafting a document. Policy-makers act on quick timescales. You will most likely only have a few hours or days (weeks if lucky) to submit a document. Don’t get caught out.
Network, network, network – A few of the initial attendees at our launch event agreed to serve on our advisory committee. Other participants later invited us to present findings at their (external) institutions. From submitting evidence to the Independent Review, John Cridland agreed to be the key-note at our policy-maker event.
Disseminate, disseminate, disseminate – Every person we met through project activities was asked if they wanted be included on our mailing list. We have a project-specific web-site and twitter account. Every published finding was sent to our mailing list, posted on the web-site and tweeted. This included our final report, titled ‘Working for Everyone’, that was written in conjunction with ILC-UK and additionally sent to their contact list as well.
Acknowledgements: Professor Jenny Head and Professor Nicola Shelton designed this impact structure. Professor Head, Dr Nicola Shelton and I planned all impact activities together. ILC-UK was instrumental in the success of our policy-maker event and report. The entire RenEWL team was instrumental in the success of our programme.
Would you let a stranger into your home? Would you then answer questions about yourself, your family and your health for an hour or so? Luckily, 10,000 people in England do so every year. Most also allow the interviewer to measure their height and weight. Many agree to a nurse visiting them later. The nurse measures their waist and blood pressure and takes blood, urine or saliva samples.
The Health Survey for England (HSE) is one of the biggest and longest-running health examination surveys in the world. It is organised by NatCen Social Research and UCL. What makes the HSE unique in the UK is that we take these measurements and we ask the general population – anyone living in a private home. We don’t rely only on questions (a ‘health interview survey’). We don’t rely only on information collected by the NHS. We work on three surveys at a time. We are currently: writing the report for the 2017 survey, running the 2018 survey, and preparing for the 2019 survey. We always obtain approval from an NHS Research Ethics Committee for the questions and measurements we plan to include before we start the survey.
Why is this important? Most people report that they are taller than they actually are, and weigh less than they actually do. Relying on self-reported information underestimates how big the obesity problem is in England. People who have undiagnosed diseases cannot tell us about them. By measuring blood pressure, we can find out how many people have high blood pressure (‘hypertension’) but don’t know it. We do the same for diabetes by measuring blood sugar levels. We also collect saliva to measure cotinine. This is made by the body when exposed to nicotine. Smokers have high levels. Non-smokers have measurable cotinine if they spend time in places where other people smoke. Although levels are much lower, it shows they are exposed to the thousands of harmful chemicals in tobacco smoke.
The HSE has been running since 1991. Some information on how health and health risk factors have changed over time has been put onto the HSE website. Obesity in children increased from the early 1990s to the early 2000s. It fell a little but is still too high. We also showed that waist circumference has increased in teenagers even more than general obesity. In adults, too, obesity increased in the 1990s to the mid-2000s. It hasn’t changed much in recent years. However, waist circumference continues to rise. This is more worrying as it is a marker of ‘abdominal obesity’, with fat collecting in the abdomen. This gives people a high risk of developing diseases such as diabetes, heart disease, or some types of cancer.
There is also good news in the health trends. The proportion of adults who smoke cigarettes has fallen from 27% in 1993 to 18% in 2016. Even where parents smoke, the proportion who try to keep their home smoke free has increased.[i] In 2006, two-thirds of non-smoking children had cotinine in their saliva, because of exposure to other people’s smoke. By 2014/15, this had fallen to just over one-third of non-smoking children. The management of high blood pressure is much better than it used to be.[ii] However, it still needs to improve further.
The Health Survey for England 2016 report provided information on many topics. 16% of children, 26% of men and 27% of women were obese. Chronic liver disease was most common in adults aged 55 to 64 years. Almost one in five adults (19%) had probable mental illness. Almost one in four adults (24%) had taken three or more prescribed medicines in the previous seven days. 66% of men and 58% of women met the aerobic physical activity guidelines.
Cases of diabetes are on the rise. Is that because more people are becoming diabetic or because doctors are better at finding those people? HSE data show that both are happening. At one time, for every diagnosed case of diabetes, there were two more people with undiagnosed diabetes. By 2013, 7% of people had diabetes. Four-fifths were diagnosed.[iii] In other words, there were eight people with diagnosed diabetes for every two who didn’t know they had diabetes. A great improvement.
UCL staff are analysing data on adult health; combinations of health risk factors; and circulatory diseases, such as heart attacks and strokes. NatCen staff are analysing data on social care; adult and child obesity; and health of children. Watch out on the UCL, NatCen and NHS Digital websites (listed below) and in the news to see what we find. And if you ever receive a letter inviting you to take part in the HSE, please do!
Professor Jennifer Mindell is a public health doctor who has also worked in general practice and health promotion. She is interested in policies outside the health services that affect health and inequalities. She leads the UCL team dealing with the Health Survey for England and other health examination surveys in the UK; comparative work across Europe (EHES); and a comparison project (ESARU) across the Americas and the UK. Prior to this, she was the Deputy Director of the London Health Observatory. She led health impact assessments (HIAs) of the London Mayor’s Transport and other strategies. She was the chief investigator for a large research project at UCL, Street Mobility. This developed tools to measure the barrier effect of busy roads and the effects on local people. She chairs the UK Faculty of Public Health’s Health Improvement Committee and sits on the FPH Health Policy Committee. She is the health lead for the UCL Transport Institute. She is also Editor-in-chief of the new, award-winning Journal of Transport and Health. She was also very involved nationally in tobacco control for many years. See Jenny Mindell’s IRIS profile web page
For more information about the Health Survey for England, visit the following websites:
[i] Jarvis M, Sims M, Gilmore A, Mindell JS. Impact of smoke-free legislation on children’s exposure to passive smoking: cotinine data from the Health Survey for England. Tobacco Control. 2012;21:18-23. https://tobaccocontrol.bmj.com/content/21/1/18
[iii] Moody A, Cowley G, NgFat L, Mindell JS. Social inequalities in prevalence of diagnosed and undiagnosed diabetes and impaired glucose regulation in participants in the Health Surveys for England series. BMJ Open. 2016;6:e010155. https://bmjopen.bmj.com/content/6/2/e010155
Doing a PhD is rewarding, but at times challenging. During my PhD, there are times when I feel I should not be there. While I was indeed struggling to get some results, other very clever students in the IEHC were doing an amazing job; they were publishing to international journals, they were writing and talking to the media about their work, and they were also attending great conferences in the UK and abroad. It was then that I started feeling an outsider in academia; that I maybe sneaked my way in and I was/am about to be found out anytime soon. This is impostor syndrome and (believe it or not) it is very common among PhD students. Paradoxically, impostor syndrome is that intrusive idea that your success is due to mere luck and not your talent or qualifications. Evidence shows that about 70% of people experience it, according to the Journal of Behavioral Science https://www.tci-thaijo.org/index.php/IJBS/article/view/521 . So far, there is no single explanation as to why impostor syndrome occurs. Some experts believe that it has to do with personality traits like anxiety or neuroticism, while others focus on family and behavioural determinants.
Working day-in day-out towards an ultimate goal; a completion of a PhD in this case was never meant to be an easy task. Many people describe PhD time as an emotional ‘’roller coaster‘’ (https://core.ac.uk/download/pdf/11233054.pdf) with many ups and downs along the way, but for some people like me, it looks to be more than that. During one of the first panel meetings with my PhD supervisors, one of them explained to me that ‘’doing a PhD would render me an expert in my topic’’. While that is true to a certain extent, living up to such an expectation (if taken literally and really did take it literally) can be very difficult. However, the good news is that impostor feelings can be managed to enable you to work to the best of your ability.
One of the first steps to start dealing with impostor feelings is to acknowledge that you have impostor thoughts and put them into perspective. Remind yourself than an impostor thought is just a thought, and not the reality.
Consider your PhD as just a beginners qualification. A PhD is the time during which you develop basic research skills, which you can further develop along the course of your professional career (academic or not). Never say never! Probably in the future you can become a prominent expert in your field, but this certainly takes much more effort and time than a three or four year long PhD.
Something that my PhD topic and experience has taught me so far is that my/your ability is not fixed, but something that can be developed and improved over time with effort and most importantly, patience. What I am always trying to remind myself of is the Socratic paradox; according to which the Greek philosopher Socrates responded to an oracle posed by Pythia, the oracle of Delphi ‘’Socrates is the wisest’’ that ‘’The only thing I know is that I know nothing’’. Truly liberating!
One thing that you can also try is to reframe your thoughts. One way to do so is to learn how to respond to challenges by learning how to value constructive criticism; that it is not a sign of academic incompetence to ask ‘’stupid’’ questions, to ask for help even for something that is considered ‘’easy’’ by others, or remembering that the more you practice a skill, the better you will get at it.
Last but not least, it can be helpful to share your feelings with trusted friends, your partner, mentors or your supervisors. When in doubt, our thoughts may be tricking us to believe in something which may not be true. Therefore, being open about your impostor thoughts may allow other people to critically assess your thoughts together and possibly de-dramatise them. People who have more experience can reassure you that what you’re feeling is normal, and knowing others have been in your position can make it seem less frightening. Nevertheless, if you think that by doing so will not make any difference, it will be wise to seek professional help. UCL’s Students Psychological and Counselling Services are doing a great job in helping students with challenging feelings such as those related to impostor syndrome, either by providing a number of one to one sessions with a therapist or by providing specialized courses on how to overcome PhD perfectionist thoughts (I have been to one of those great courses and they really do help a lot).
To conclude, if you have impostor thoughts, it is important to remember that most people experience moments of doubt, and that is completely normal and not something to feel bad about it. The main goal should not be for you to not have impostor related moments, but not an impostor life. No matter how much effort and time it takes, the impostor syndrome can effectively be managed and overcome.
Lots of studies have suggested stress can be a cause of ill health – and that leads to people ceasing to work before they reach retirement age. But most have offered only a snapshot on the issue. José Ignacio Cuitún Coronado and Tarani Chandola from the University of Manchester describe a major new study, which has shed new light on how work stress can affect an employee’s health over a longer period.
Many animals have the ability to adapt to environmental changes and pressures so that they’re better prepared the next time they happen. Bears can put on fat as winter approaches, for instance, to help them stave off hunger and stay warm.
And human beings can do this too. Stressful situations trigger chemical responses which can help to give us extra resources when things are tough. Our neuroendocrine systems, for instance, trigger hormonal responses which enhance our physical performance when we need it most.
But these valuable systems can have a down-side. In our research, we wanted to look at how repeated exposure to stressful situations might contribute to health problems, particularly in people nearing the end of their working lives. We call this stress-induced effect ‘Allostatic Load’ – the “wear and tear” on the body that accumulates as an individual is exposed to repeated or chronic stress because of fluctuating hormonal responses.
Given that many governments are looking for ways to extend working lives, there’s particular interest in finding out how stress can affect the health of older workers. We were able to tap into a rich source of information – the English Longitudinal Study of Ageing (ELSA), which has followed a representative sample of almost 10,000 over-50s since 2002.
These participants have been interviewed regularly and one of the things they’ve been asked to report is whether they’ve experienced a sense of imbalance between the effort they put into their jobs and the rewards they get out.
This gave us a sample of 2663 older adults, all over 50 and living in England, who’d reported these feelings at least once and who’d been assessed as having had an adverse reaction to them. We wanted to know whether repeated episodes had a bigger effect than just one, and whether the effect would be just as strong for past episodes as it was for more recent ones.
Health testing
Between 2004-5 and 2014-16 the group were asked about stress at work, but they also underwent physical tests to see how the various systems in their bodies were bearing up.
They were visited by nurses who carried out a battery of tests including taking hair samples to assess levels of the stress-related hormone cortisol, carrying out blood pressure checks to provide information on their cardio-vascular systems, white blood cell counts to assess their immune systems and cholesterol checks on their metabolic systems. Participants also had measurements taken of their waist to height ratios – a good indicator of coronary heart disease risk factors.
Overall, we found the more occasions of work-stress a participant had reported, the greater their ‘Allostatic Load’ index – that is, the greater the amount of biological wear and tear.
Moreover, the evidence suggests that employees who had experienced stress more recently, towards the end of their working lives, had higher levels of health risk when compared to those who had experienced it earlier in their careers.
This suggests there is an association between repeated reports of stress at work and biological stress mechanisms, which in turn could lead to stress-related disorders such as coronary heart disease, type 2 diabetes or depression. This also suggests that previous cross-sectional studies which reported small or inconsistent associations may have suffered because they were only measuring one effect at one time.
Work-related stress is one of the reasons for labour market exit – and our findings would suggest that earlier, snapshot studies may have underestimated the true effect of work-related stress on health over a lifetime.
As this is an observational study, we cannot make any causal claims. There may be other factors that we have not taken into account that may explain the association between stress and disease risk. For example, sleep problems may be relevant – though they may also be part of the journey from stress to ill-health.
But equally it is possible that cumulative exposure to work stress is resulting in damage to employees’ physical health, which is then leading to disability and an early exit from the world of work. So, if we want to extend working lives then reducing work-related stress could be one of the keys to achieving that goal.
This blog article is courtesy of the Work Life blog, which is a blog about the relationship between work and health and well-being of people, whether they are preparing for working life, managing their work / life balance or preparing for retirement and life beyond retirement. Led by the ESRC International Centre for Lifecourse Studies, University College London
Across the developed world, a growing share of the population suffers from chronic disease such as diabetes, arthritis or heart problems – in the EU, around 45 per cent of those aged 55-64 had such a disease in 2015. And that affects their ability to work: just half of those with chronic illnesses are employed, compared to three quarters of those without. But how do the self-employed cope with such conditions, when compared with those in employment? Maria Fleischmann and colleagues from the RenEWL project find these differences in work status can make a major difference.
We know that when people become chronically ill, changes in their working conditions can help them to continue working. And we also know that good working conditions – being able to control how you use your time and how you do your job, whether you make the decisions and whether you feel valued, for instance – can help all of us to stay in paid work for longer.
And of course, if you become ill you’re more likely to feel the need to take time off or maybe to give up work altogether. We wanted to compare how the employed and the self-employed adjust their working conditions when facing a diagnosis of chronic disease.
Existing research tells us that many older people work for employers, and have to ask for their approval when it comes to making adjustments to their working conditions. The self-employed, meanwhile, are much more able to make their own decisions and tend to feel they have more control over their working lives.
We looked at people’s ability to control their work: physical demands, working hours, psychological demands such as how fast they had to work, and social aspects such as whether they felt valued.
And we had a great source of data for this – the English Longitudinal Study of Ageing (ELSA), which has followed a total of almost 9,000 over-50s since 2002.
From that group we were able to find and study 1389 participants who reported no chronic diseases when they were interviewed in 2004-5 – the second wave of interviews – and who were in work. We were then able to look at what happened to them before the seventh wave of interviews, in 2013-14.
A little over 40 per cent of our sample were in managerial or professional occupations, a quarter in intermediate occupations, and almost 30 per cent in routine and manual occupations.
After diagnosis
At each interview, respondents were asked whether they had been diagnosed by a doctor with lung disease, asthma, arthritis, cancer, high blood pressure, diabetes or high blood sugar, stroke or heart problems.
During the study period 510 of the 1389 sample members were newly diagnosed with one of those conditions. We were able to look at how they fared at work for four years after that, and we found some striking differences between how the employed and the self-employed seemed to have been treated.
The physical demands of our participants’ jobs were pretty similar before their diagnosis, for instance. But afterwards significant numbers of those who were employed said that those demands had actually increased when they were diagnosed. The self-employed, meanwhile, told us the opposite had happened to them – they reported significantly lower physical demands at work immediately after diagnosis. This effect continued for some time, though it grew less pronounced.
How could that be? We think maybe the increase in physical demands among the employed could be due to perception – similar demands might be perceived as more strenuous by the chronically ill. The self-employed, meanwhile, have more freedom to adjust those demands when they feel they need to.
The self-employed reported that their working hours dropped by an average of 2.8 hours per week on diagnosis, while those who were employed did not see a change. This effect was not statistically significant, though.
Employees found that their level of autonomy at work also dropped marginally, while for the self-employed there was no significant change. We did not find any major changes in psychological or social conditions in either group.
So, what did we learn? Essentially, that improvements in working conditions after diagnosis of chronic illness were restricted to the self-employed. So employers may need to ask themselves some hard questions – do they want to hold on to workers who become unwell? If they do, then they should consider the levels of flexibility they offer, and they should think about making adjustments for those workers if they don’t want to lose them.
In an ageing society, older people are expected to work ever longer and therefore to remain at work even when they begin to suffer from health problems. Our findings should also encourage policy-makers and governments to think about how chronically ill older adults are treated at work.
This blog article is courtesy of the Work Life blog, which is a blog about the relationship between work and health and well-being of people, whether they are preparing for working life, managing their work / life balance or preparing for retirement and life beyond retirement. Led by the ESRC International Centre for Lifecourse Studies, University College London,
Internships are increasingly being seen as a valuable addition to PhD training. In fact a report commissioned by the Government recommended that, “All full‐time PhD students should have an opportunity to experience at least one 8 to 12 week internship during their period of study” (Wilson Review, 2012, p.8). But how do you go about getting one? And how do you convince your supervisors if they’re not so keen? Fran Harkness, PhD student at the MRC Unit of Lifelong Health and Ageing lets us in on her insights.
I did an internship in the MRC External Affairs team March-June this year. I enjoyed it so much that I’ve since been asked if I’m being paid to persuade other students to go on one by demonic internship overlords? Anyway, as I had to do the hard work of understanding how to get one, I hope that I’ve managed to clarify the process a bit for you. Good luck!
Research it. Think about what you want to get out of this time. I was interested in science policy so it made sense to apply to the Academy of Medical Sciences policy internship scheme. Research councils have links with many organisations. You could intern with the Royal Institution to plan their Christmas lecture. The UKRI scheme sponsors students to get insight into areas as diverse as the civil service, Age UK, and Public Health England. Alternatively you could apply for funding to work in a research unit abroad to pick up new skills and ideas in your own field.
Take time over your application. You need to collate your CV, a statement of interest, and often a fresh piece of work, plus signature from your supervisor. I’d broach the latter first. Don’t do what I did once and stall asking your primary supervisor for so long that it’s now the day of admission and she surprisingly isn’t looking at her emails in Chamonix. That was after I’d spent, I mean wasted, five days writing a government POST note far out of my subject area for the application. On my second application I’d mortifyingly left in a note to myself in blank space after my essay. Proofreading doesn’t take that long.
Convince your supervisors part 1. My stalling behaviour was partly fuelled by anxiety that mine would say no. Your supervisors want to support you to finish on time and may believe that an internship will derail this ambition. Many schemes include a funded extension but their worry is that any absence breaks your flow and delays finish time. Reassuringly, researchers from the University of California found that interns don’t take any longer to graduate, despite halting their programme entirely during the three months. My experience has been that my internship returned me to a mental state helpful for finishing: professional, confident and newly reminded of the point of my research.
Convince your supervisors part 2. Like being asked by my parents to plan how I was going to take the bus into town by myself for the first time, my panel had kindly reservations for me to consider. They requested that I talk to previous interns about the benefits and challenges and how I would overcome the latter. They also asked that I continue to work on my thesis during my internship and that I take it up towards the end of my PhD so that there wasn’t too much write-up hanging over my head. Those last two things didn’t end up happening, but by this time I’m already on the bus into town and nobody minds.
Apply! With your head stuck in a stats problem or down a microscope you may forget that you have time for an internship. Look up and remember that your PhD is a training opportunity for the real world. You can gain new skills, meet contacts, and learn of roles you didn’t realise existed. It can help you get a job afterwards. At the Academy of Medical Sciences every single policy advisor I spoke to had done an internship there during their PhD. I know someone whose internship was so successful she’s now working part time for that organisation whilst finishing her PhD. On top of all this they’re great fun. Go on!
 Close
Close









 The
The  Doing a PhD is rewarding, but at times challenging. During my PhD, there are times when I feel I should not be there. While I was indeed struggling to get some results, other very clever students in the IEHC were doing an amazing job; they were publishing to international journals, they were writing and talking to the media about their work, and they were also attending great conferences in the UK and abroad. It was then that I started feeling an outsider in academia; that I maybe sneaked my way in and I was/am about to be found out anytime soon. This is impostor syndrome and (believe it or not) it is very common among PhD students. Paradoxically, impostor syndrome is that intrusive idea that your success is due to mere luck and not your talent or qualifications. Evidence shows that about 70% of people experience it, according to the Journal of Behavioral Science
Doing a PhD is rewarding, but at times challenging. During my PhD, there are times when I feel I should not be there. While I was indeed struggling to get some results, other very clever students in the IEHC were doing an amazing job; they were publishing to international journals, they were writing and talking to the media about their work, and they were also attending great conferences in the UK and abroad. It was then that I started feeling an outsider in academia; that I maybe sneaked my way in and I was/am about to be found out anytime soon. This is impostor syndrome and (believe it or not) it is very common among PhD students. Paradoxically, impostor syndrome is that intrusive idea that your success is due to mere luck and not your talent or qualifications. Evidence shows that about 70% of people experience it, according to the Journal of Behavioral Science 


