Close
Close

Extraordinary Eaters: Swallowing Foreign Objects for a Living
By Gemma Angel, on 22 April 2013
 by Sarah Chaney
by Sarah Chaney

In 1935, Dr Isaac Lloyd Johnstone decided to publish a “case of unusual surgical and psychological interest” in the British Medical Journal. This concerned a patient he had encountered over a decade before, while he was a surgical dresser at the Middlesex Hospital. This man was operated on for the removal of several nails and, as Lloyd Johnstone took the patient’s medical history, he discovered that his abdomen was “a mass of scars”; the patient described having had more than a dozen similar operations in the past. Before leaving the hospital, the patient had handed the dresser his memoirs, intriguingly titled “Things I have swallowed since 1905”.[1]

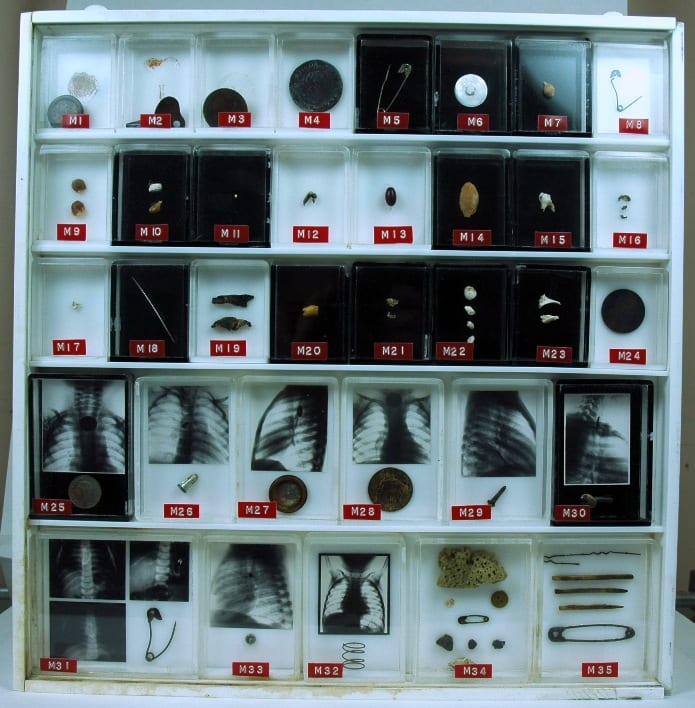
Foreign bodies removed from the stomach of a 26-year-old woman in 1915, The Museums at the Royal College of Surgeons.
The patient’s account described around a dozen operations for the removal of items, predominantly nails, screws and cutlery, but also hairpins, safety pins and, once, a tin whistle. According to Lloyd Johnstone, his informant would make money from his ability to swallow unusual items, by showing a group of objects to his companions in various public houses, and taking wagers against his ability to swallow them. The patient stated that he had always been able to pass objects up to two and a half inches in length, and Johnstone considered that larger objects found their way into the patient’s abdomen when “a drink or two and an intimate knowledge of the hospitals of London made him reckless”.
Indeed, the wagers did not necessarily end with the initial swallowing. In 1912, the patient reported having wound up in Guy’s Hospital after swallowing a 6 ½ inch nail, which took three operations to remove. In his own words:
Before being operated on there was a bet between the Night Nurse and the Student as were the 6 ½ inch lied, one said it was in the transfered Coln, and the Night Nurse said it layed in the Coln, to make sure Mr. John Dunn had me X Rayed and Skiagraphed and the Skiagraph showed that it was in the Coln, and then I was operated on straightaway. The Night Nurse won the Bet which was £5 0, 0 which my Dresser Mr. Taylor had to pay up. [sic]
In Mr XYZ’s account (as Lloyd Johnstone called him), the bet is emphasised over and above his own recovery, indicating the importance he laid on this aspect of his swallowing. The patient remained proud of his abilities, despite the painful and dangerous nature of his career. On at least one occasion, his actions had been thought fatal by hospital staff (after “6 Larg Safty Pins and 5 Ladies Hair Pins … they gave me up for Dead”), yet his account ends proudly with the words “I defy contradiction”. His composure and purpose, as Lloyd Johnstone noted, made XYZ very different from the “usual” hysterical or suicidal cases of foreign body ingestion.
Yet swallowing objects for money or notoriety has a lengthy history, bound up in the notions of performance and risk covered in a previous blog post on sword swallowing. Historian Emma Spary has researched the connections between the medical profession and the swallowers often referred to as “extraordinary eaters”. Her recent book – Eating the Enlightenment – includes a chapter on the involvement of the medical profession in cases of the consumption of non-nutritive items in 18th century Paris.[2]

The contents of the stomach of a knife eater, Gordon Museum (King’s College London)
One such case which features in a London museum is the “contents of the stomach of a knife eater”, housed in the Gordon Museum. This collection of rusty blades, buttons and medallions was removed by surgeons at Guy’s Hospital from the stomach of an American seaman named Cummings, known to the British medical profession from 1799. This unfortunate individual (much like the sword swallower in the UCL collections) ended up being dissected by surgeons a decade later. Like Mr XYZ, Cummings reminds us that the swallowing of foreign items is not necessarily an irrational pursuit, and might be carried out for a wide variety of reasons.
You can watch a video of Dr Spary discussing “extraordinary eaters” on the Damaging the Body website here.