 Close
Close

Health messaging to encourage key protective behaviours to reduce the spread of Covid-19: What we can learn from existing evidence about getting the message right?
By Nathan Davies, on 7 May 2021
In this months post Dr Sadie Lawes-Wickwar, a Health Psychologist and Lecturer in the department teamed up with other health researchers, health psychologists, public health practitioners, and public contributors across the UK during the COVID-19 pandemic to find out what we can learn about getting the message right to support the public to prevent the spread of Covid-19.
In the event of an outbreak of an infectious disease, the population is required to make often rapid changes to their behaviour to reduce the spread. Public health campaigns can support population-level behaviour change, but it is crucial that the public receives consistent, clear information, so they understand what it is they need to do new (e.g. when using fa
ce coverings). However, public information during a pandemic can be conflicting, change frequently, or use language that the general population may find it hard to understand. We need to think
carefully about the messages that are used to instruct the public to perform behaviours that are key to reducing the spread of a virus.
After the outbreak of Covid-19 in the UK last year, a collaborative group of health psychologists, behavioural scientists, public health practitioners, and members of the public formed the Health Psychology Exchange to support the public health response to the pandemic. A group of Health Psychology Exchange members set about reviewing existing evidence to inform recommendations for local and national public health teams in developing health campaigns. Our aim was to identify what characterises effective public health messages for managing risk and preventing infectious disease, and what influences people’s responses to such messages.
Our first review of public health messaging found that, to influence behaviour effectively at the population level, messages need to be acceptable to the populations they are targeting, be delivered by credible and trustworthy sources, and in language target populations can understand, to increase understanding and threat perceptions [1]. Specifically, in the context of encouraging vaccine uptake, evidence tells us that providing information about virus risks, vaccination safety, vaccine clinics, and addressing misunderstandings about vaccines, can support uptake at hospitals (e.g. among hospital staff) or within local communities. We can also support understanding and beliefs about vaccines by framing messages in a particular way, such as emphasising the reduction of risks and the benefits to society from being vaccinated [2].
Our work has highlighted gaps in research and the development of previous public health messages, including the valuable input of the public in the design, delivery, dissemination and evaluation of health messages [2]. One of our key recommendations has been the involvement of local communities in all aspects of the messaging process, which is also in line with recommendations from the World Health Organisation (WHO)[3]. We also need more high-quality research to demonstrate the effects of messaging interventions on the uptake of recommended behaviours. Surprisingly few studies to date have evaluated messages adequately to be able to conclude the definitive impact of campaigns on population-level behaviour, such as vaccine uptake.
Our recommendations have informed two British Psychological Society (BPS) Behavioural Science Disease Prevention Taskforce guidance documents to date, one to support public health teams to deliver effective public health campaigns, and another to optimise vaccination uptake during Covid-19. Using behavioural science can boost public health campaigns during the Covid-19 pandemic, and I hope to see more collaborations between health psychologists and public health teams in the coming months as we look to a brighter future.
- Ghio, D., et al., What Influences People’s Responses To Public Health Messages For Managing Risks And Preventing Disease During Public Health Crises? A Rapid Review Of The Evidence And Recommendations. PsyArXiv Preprints, 2020.
- Lawes-Wickwar, S., et al., A rapid systematic review of public responses to health messages encouraging vaccination against infectious diseases in a pandemic or epidemic. Vaccines, 2021. 9(2): p. 72.
- WHO, Communicating risk in public health emergencies: a WHO guideline for emergency risk communication (ERC) policy and practice. 2017: World Health Organization.
Destabilising primary healthcare: Digitalised remote consulting and post- COVID-19 patient care
By Nathan Davies, on 28 September 2020
Sophie Park1, Yathavan Premadasan1, and Chris Salisbury2
Sophie Park MBChB M.Med. Sci (dist) FRCGP SFHEA, EdD. Professor of Primary Care and Medical Education. sophie.park@ucl.ac.uk
Yathavan Premadasan, BSc. Medical Student, University College London. zchaypr@ucl.ac.uk
Chris Salisbury, MBChB, MSc, MD, FRCGP. Professor of Primary Health Care, University of Bristol. c.salisbury@bristol.ac.uk
1 Research Department of Primary Care and Population Health, UCL, Royal Free Campus, Rowland Hill St. Hampstead, London NW3 2PY
2 Centre for Academic Primary Care, Bristol Medical School, University of Bristol. Canynge Hall, 39 Whatley Road, Bristol BS8 2PS
The COVID-19 pandemic has changed Primary Care dramatically(1), with most consultations conducted remotely by telephone, video or online messaging. But is this a short-term adjustment or the future norm? In General Practice, clinical care has been based on long term face-to-face contact, establishing trusting relationships through continuity of care, and using knowledge of patients’ personal circumstances and social context to provide holistic support. Now, these fundamental principles are challenged.
Matt Hancock (UK Health Secretary) has welcomed rapid changes towards digitalised clinical practice as an overdue development, stating that wherever possible, all future consultations should be conducted remotely(2). But is the pandemic ‘crisis’ simply being used to introduce unscrutinised change? The WHO recently considered the opportunities and challenges of digitalising healthcare systems(3) to address global healthcare workforce shortages and support delivery of universal healthcare, interprofessional working and patient engagement. The report also highlighted potential challenges to equality and social justice posed by private companies keen to exploit the healthcare “market”.
Accessing healthcare through digital services initially seems cheap and even democratizing – what could be easier than emailing your GP? But the reality can be very different. It potentially undermines core primary care principles: the importance of patient interaction; treatment of the whole patient; and situated use of evidence to individualise care, for example negotiating competing priorities in the context of multimorbidity. Worse, it widens health inequality: the healthy, the wealthy and those requiring simple transactional interactions benefit; whilst those with complex health problems struggle to get the care they need.
Remote digital consultations work well for simple transactions(4), for example, where a straightforward problem leads to a clear-cut disease diagnosis and treatment. But the main users of Primary Care are young children, the elderly, and those with multiple problems associated with long-term health and social conditions. Telephone and video provide less rich information than face-to-face consultations, making management of these complex situations difficult(4). The move towards remote consultations is a shift towards less personal and more transactional healthcare and away from an individualised, whole-person approach built on a patient-doctor relationship. Using an online form or telephone consultation means problems risk becoming over-simplified, over-investigated, medicalised and stripped of context and nuance. There is less opportunity for in-depth exploration of patients’ concerns and health beliefs, or for shared decision-making.
Studies in different countries have consistently shown that patients choosing remote consultations are predominantly young adults who are healthier, more educated and more affluent than average(5,6). These are the opposite of the characteristics associated with health need. Older, less educated patients and those with chronic illness are motivated to access digital healthcare, but face more difficulties in doing so because of lack of access to technology, the confidence and skills to use it, or physical or cognitive limitations(7). This should be no surprise to those looking at the “digital divide” in other sectors. For example, over 1 million Lloyds Bank customers (16%) required help to access internet and digital services; moving universal credit on-line increased claimants’ use of Citizens Advice; and, it is the over-75s who comprise most internet non-users(8).
Digitalised access to healthcare does not therefore equate to equitable access, nor does it necessarily reduce professional workload(9). Digital access can increase demand, as a ‘quick and convenient’ patient option(6) and can increase the need for follow-up(10).
These changes impact how primary care is perceived. For patients, those with simple health needs may appreciate the convenience of remote consulting but those with important personal issues to discuss may resent barriers to seeing a doctor in person. For GPs, it can undermine their sense of purpose and identity(10): many doctors choose to work in primary care because they want to offer high-quality, holistic care to a patient they know. If a large proportion of their day is spent emailing or telephoning unfamiliar patients, it degrades both the quality of care and satisfaction in their work. Doubtless it will influence career choices of future doctors.
Short-term, we need to make patient care during the pandemic safe. This requires dynamic and personalised risk-assessments with patients to ensure that face-to-face contact is only used when clinically needed, and in the patients’ overall best interests. While more remote consultations are needed, teams can maximise collaborative learning about how best to conduct and utilise digital patient interactions. However, we should resist normalising remote-first healthcare in the longer-term. Remote consultations offer advantages in specific situations. ‘Digital First’ interactions remain, however, problematic for many patient groups and long-term strategies need to retain agile, flexible and human-centred services, enabling patient choice about access and quality of care.
References
- Webster P. Virtual health care in the era of COVID-19. Lancet. 2020;395(10231):1180-81. doi: 10.1016/S0140-6736(20)30818-7
- ‘More Zoom medicine needed’ in NHS says Hancock: BBC; 2020 [Available from: https://www.bbc.co.uk/news/health-53592678 accessed 28/08/2020.
- ‘Future of Digital Health Systems: Report on the WHO Symposium on the Future of Digital Health Systems in the European Region’. Copenhagen, Denmark 6-8th February 2019. World Health Organisation (Regional Office for Europe).
- Hammersley V, Donaghy E, Parker R, et al. Comparing the content and quality of video, telephone, and face-to-face consultations: a non-randomised, quasiexperimental, exploratory study in UK primary care. Br J Gen Pract 2019;69(686):e595-e604. doi: 10.3399/bjgp19X704573
- Rodgers M, Raine G, Thomas S, et al. Informing NHS policy in ‘digital-first primary care’: a rapid evidence synthesis. Health Services and Delivery Research 2019;7(41) doi: 10.3310/hsdr07410
- Pearl R. Kaiser Permanente Northern California: current experiences with internet mobile, and video technologies. Health Aff (Millwood) 2014;33(2):251-7. doi:10.1377/hlthaff.2013.1005
- Nijland N, van Gemert-Pijnen JEWC, Boer H, et al. Increasing the use of econsultation in primary care: Results of an online survey among non-users of econsultation. Int J Med Inf 2009;78(10):688-703. doi: 10.1016/j.ijmedinf.2009.06.002
- Elahi F. Digital Inclusion: Bridging Divides: Cumberland Lodge; 2020 [Available from: https://www.cumberlandlodge.ac.uk/read-watch-listen/digital-inclusion-bridgingdivides-cumberland-lodge-report accessed 28/08/2020.
- Salisbury C, Murphy M, Duncan P. The Impact of Digital-First Consultations on Workload in General Practice: Modeling Study. Journal of medical Internet research 2020;22(6):e18203. doi: 10.2196/18203
- Atherton H, Brant H, Ziebland S, et al. The potential of alternatives to face-to-face consultation in general practice, and the impact on different patient groups: a mixed methods case study. Health Services and Delivery Research 2018;6(20) doi: 10.3310/hsdr06200
Contributors
All authors contributed to the conception and design of this blog, and YP undertook searches of relevant literature. SP and CS drafted the manuscript and YP commented on and approved it.
This blog was originally posted on the NIHR School for Primary Care blog.
UCL Medical School Leading the UK Culinary Medicine Teaching Movement
By Nathan Davies, on 21 September 2020
 In this post, Jessica Xie (final-year UCL medical student) shares why UCL medical students have been swapping their scrubs for aprons for an eventful day of learning in a teaching kitchen.
In this post, Jessica Xie (final-year UCL medical student) shares why UCL medical students have been swapping their scrubs for aprons for an eventful day of learning in a teaching kitchen.
Nutrition education in the first three (pre-clinical) years of the UCL undergraduate medical (MBBS) curriculum includes nutritional science and public health nutrition. In every medical specialty from Paediatrics to Geriatrics, there is increasing evidence to suggest that nutrition plays a central role in determining morbidity and mortality. Thus, it is increasingly important for students to learn about nutrition in a clinical context.
The aims of the course are to equip students with the knowledge and skills to recognise patients whose health and wellbeing may be improved through dietary modification, and to be able to provide basic dietary advice.
Set in a teaching kitchen at Westminster Kingsway College, the course provides a unique learning experience. Students engage in a variety of teaching methods, including an online module, face-to-face tutorials, case-based discussions, role play and culinary skills training. Topics that have been taught on the course so far include types of diet and their evidence base, dietary interventions to treat or as an adjunct for disease management and socioeconomic determinants of dietary patterns and access to food. The skills that students gain from Culinary Medicine teaching include food identification and preparation, and communication skills, including motivational interviewing (MI). The latter is the art of empowering an individual to change their behaviour to achieve health and wellbeing improvement. A doctor’s role in MI is to highlight to patients aspects of their lifestyle that could be improved, collaborate with patients to create achievable goals and to support patients to make, and sustain, the behaviour change(s) themselves.

A nutritious meal cooked by UCL medical students during the Culinary Medicine course kitchen session.
Since March 2020, teaching has been delivered online via Blackboard Collaborate and new topics have been introduced to educate students about nutrition challenges exacerbated by COVID-19, for example access to food. One such topic is Nutrition Insecurity which is centred around a case study which highlights the disproportionate effect of COVID-19 on ethnic minorities, people of low socioeconomic status and those with pre-existing co-morbidities. Not only do students have the task of considering nutrition priorities from a patient’s perspective, they must also produce an appropriate management plan that addresses both the patient’s health and social needs. This task increases students’ understanding of socioeconomic determinants of health and emphasises the importance of an interdisciplinary approach to health and wellbeing.
In June 2020, the UCL Primary Care team and CMUK organised a live cook-along webinar, led by CMUK founder (Dr Rupy Aujla) and Culinary Lead for CMUK (Chef Vince Kelly). Recipes were created using ingredients that are typically found in food bank parcels and were emailed to students in advance to encourage participation. The two hosts had a cook-off with Chef Vince producing an impressive four-course meal that won the majority of students’ votes, securing his victory!
In future teaching sessions, students can look forward to webinars on culinary skills training, motivational interviewing role play and Q&A sessions with patients about their experiences of nutrition in healthcare. The topic Food Sustainability will also feature to teach students how to eat well whilst reducing their carbon footprint.
Elements of nutrition education will be woven into other aspects of the MBBS curriculum. For example, students will be encouraged to incorporate nutrition advice into their General Practice reflective essays about a patient with chronic disease.
The UCL Culinary Medicine course was recently featured on BBC London news for being an innovative method of teaching medical students and doctors about clinical nutrition, and is endorsed by chefs and celebrities.
With thanks to Dr Sara Thompson for her input in writing this blog post.
Covid 19: Adapting to new realities and ensuring well-being
By Nathan Davies, on 21 September 2020
By Dr Patricia Schartau
The Covid 19 pandemic is likely one of the most consequential global challenges of this generation. Individually, it impacts on all aspects of our lives including our health, finances, relationships, wellbeing and sense of self. Globally, it has far reaching consequences by affecting our healthcare systems, the economy and the way our world functions on an everyday level.
While this is a new type of ‘disaster’, for decades researchers have mapped the phases of emotional response to crisis, such as natural catastrophes and terrorism1: The initial ‘heroic’ phase2 is characterised by high levels of activity and a surge in altruistic behaviours (e.g. volunteering, healthcare workers stepping up). The ‘honeymoon’ phase which followed through April3 comprised a sense of collective optimism and virtual community bonding. In May the ‘disillusionment phase’ started, probably the most challenging phase characterised by a heightened sense of discouragement and stress. This phase is associated with negative emotions, such as anxiety and sadness, and physiological upsets such as insomnia, dream disturbances and hyperarousal. Eventually, we will progress into a calmer yet similarly challenging phase, the ‘reconstruction’ phase. Whilst some of the phase headings seem somewhat misleading given the gravity of the situation and it is important to recognise the fluidity of the phases, they provide a good framework in order to describe human emotions and behaviours in response to crisis.
The ‘disillusionment’ phase, our current phase, exposes our vulnerabilities- our respective roles amongst family and friends, in employment and the wider society have been shaken up. The fragility of our health, wellbeing and socio-economic security have been exposed. What seemed relatively untouchable (e.g. freedom of movement, supply chains of medications and food) suddenly collapsed. Whilst the world around us moved and reformed on a daily basis, our own personal tsunamis (in my case primarily the unexpected loss of a close family member and losing some of my patients to Covid 19) create even more instability, with the usual safety nets, such as social activities and work routine, having become disabled.
Over the past months, most of us will have felt at least intermittently overwhelmed and asked ourselves- how can I make sense of this situation let alone get through it? Personally, I reflected on my PhD in emotion regulation and assimilated the public advice from former psychology colleagues, such as Willem Kuyken from Oxford University. He highlighted4 a few simple mechanisms to help cope with this challenging situation:
Focussing our attention: We naturally focus our attention to threats in order to protect ourselves. Attending to the 24/7 Covid news is cognitively and emotionally exhausting. Whilst most of us are feeling a sense of loss of control, training ourselves to re-focus (e.g. by using mindfulness techniques5) and by choosing carefully what to attend to is a way to regain it. One practical example is to limit the number of times per day we read the news and/or Covid related WhatsApp threads.
Changing how we relate to the crisis: Us humans naturally enjoy to ‘time travel’- switching from past, to present, and to the future with an incredible speed and fluidity. Making future plans keeps us goal-orientated, grounded and emotionally stable. However, during the pandemic, trying to make plans has been an additional source of distress, unsettlement and anxiety. In my experience, digesting the world in smaller bites, with a sense of calmness and patience whilst not reacting to every change around us (including one’s own emotions), helps enormously. The notion that one can change thoughts and emotions in this situation by shifting focus, and choosing personal ways to relate to the crisis, is immensely empowering and somewhat reassuring. Whilst the world out there continues to change ever so quickly, it allows to regain some much needed stability.
Taking care of ourselves and having meaningful relationships with others: This is not rocket science, but wellbeing is supported by a healthy diet, plenty of exercise, a good sleep hygiene, good hydration, keeping some kind of routine and doing things that we enjoy and that give us meaning. The latter includes social interactions with, for example, friends and family.
As Kuyken highlighted, ‘psychology offers ways for us to meet such crisis with courage, clarity and wisdom’. It also offers us alternative interpretations: For example, to value the opportunity that has arisen from the quarantine to re-evaluate personal goals and priorities:
References:
- Carson, J., Eyre, H. & Lavretsky, H. (2020). Dear Mental Health Innovators: The Covid-19 honeymoon is over. Letter in: MJH Life Sciences and Psychiatric Times.
- DeWolfe, D.J. (2000). Training manual for mental health and human service workers in major disasters. US Department of Health and Human Services. Substance Abuse and Mental Health Services Administration: Center for Mental Health Services.
- Washington, E. (2020). Phases of Disaster. https://www.samhsa.gov/dtac/recovering-disasters/phases-disaster
- Kuyken, W. (2020). Waking up in the time of Corona: four insights from Psychology.
- Kuyken, W. (2020). Keeping a cool head and warm heart in challenging times. https://www.oxfordmindfulness.org/news/keeping-a-cool-head-and-warm-heart-in-challenging-times-by-willem-kuyken/
The consequences of Covid-19 for health policy in England
By Nathan Davies, on 12 August 2020
In this Post Steve Iliffetalks about how Covid-19 has changed the NHS and health policy in England.
 The new coronavirus that arrived in the UK in January 2020 has triggered changes in the NHS which will be difficult to reverse, at least in the short to medium term. Crises lead to change when three conditions are met: there must be a latent desire for change, plus capacity to change, which pre-date the crisis; the crisis needs to reinforce the arguments for change, and even pre-figure new ways of working; and a political alliance is needed to turn the possibility of change into reality1.
The new coronavirus that arrived in the UK in January 2020 has triggered changes in the NHS which will be difficult to reverse, at least in the short to medium term. Crises lead to change when three conditions are met: there must be a latent desire for change, plus capacity to change, which pre-date the crisis; the crisis needs to reinforce the arguments for change, and even pre-figure new ways of working; and a political alliance is needed to turn the possibility of change into reality1.
In the beginning
The place and funding of Public Health as a discipline became a hot topic in the coronavirus debate as public health experts gave differing views of how to manage the pandemic. The ‘herd immunity’ view (building up a protective sub-population of the immune) was favoured initially, on the grounds that testing as many as possible of the whole population was impractical. The ‘herd immunity’ view gave way to the World Health Organisation’s strategy of mass testing in mid-March, but there were political as well as scientific reasons for this change.
Public Health, taken into the NHS from local government in 1974, was restored to local government control in the Lansley Reforms of 2012. Like the rest of local government, it has experienced substantial cuts in its budget over the last decade. Public Health has been under-resourced and the adoption of ‘herd immunity’ strategy reflected the inability to mobilise the resources needed for mass testing and contact tracing. National government has therefore opted for the second-best option of mitigating (but not controlling) the effects of COVID-19, in a country in which successive governments have deliberately underfunded Public Health services.
Changing strategy
Although it still has its advocates, the herd immunity strategy failed. The government turned to mass testing combined with containment measures (social distancing and closure of public spaces) as the optimal method for containing the pandemic. The change in strategy did not alter the problem of limited resources. Accident and Emergency departments were struggling with high levels of demand before the pandemic’s arrival, there were (by one estimate) 100,000 job vacancies across the health service, and historically the NHS had spent relatively little on intensive care facilities or staff.
An attempt to mitigate the impact of the virus by promoting voluntary action by individuals reflected not only the Conservatives’ ideological hostility to “big government” but also a belief that most people could be nudged (but not coerced) into following public health advice. This optimism ignores the evidence that people in affluent and individualistic societies easily adopt an ‘eat, drink and be merry’ culture, breaching social distancing (and other health preserving) rules as they do so.
The epidemiological modelling of Covid-19’s spread began to alarm politicians. They abandoned voluntary restraints on movement and gathering and imposed a more stringent “lock down” designed to slow virus spread and reduce demand for hospital care for those whose infection became life-threatening2.
A shambles
A seven-week delay in introducing containment measures – a delay described by one academic as “near criminal negligence” and “obfuscation”3– resulted in recurrent shortages of Personal Protective Equipment (PPE) which provoked angry responses from NHS staff. The TV image of the Health Secretary loading boxes into a van showed what a shambles NHS supply had become. The Health Care Supply Association admitted to a “system” failure, but without naming names or pointing fingers. According to the Health Service Journal some trusts turned to alternative suppliers to source protective kit, including DIY shops. Staff working in central purchasing teams reported particular difficulties in getting hold of PPE, including a lack of UK-based manufacturers, other countries restricting exports in order to meet their local demand, poor quality products arriving as buyers worked in a hurry, and some unjustified price rises introduced by suppliers. In some places protective kit was delivered to the NHS by army lorries.
Similar problems appeared once the government had changed strategy and promised widespread screening; screening tests were not available and university laboratories that could have contributed to test analysis had been mothballed and their staff sent home as part of university lockdowns 4. NHS plans to test were poorly executed. On 2nd April, The Times ran the front page headline “Virus testing plans in chaos” over an image of a large drive-through testing centre at Chessington World of Adventures at which nobody was being tested.
NHS takes control
The NHS then demonstrated what a real command-and-control management style could look like in a huge institution made up of intertwined and sometimes competing bodies. Some of these management actions may prefigure or bring about future changes. They include:
- Commissioning NHS England took over commissioning services from Clinical Commissioning Groups (CCGs), which had anyway failed to transform the ways in which the NHS worked over the preceding decade. There was latent desire for change and the crisis required the NHS centre to work around CCGs. It seems unlikely that the CCG form of commissioning will be restored.
- General Practice The NHS increasingly dictates the terms under which the public contact their GPs, encouraging doctor-patient communication via video consultations and email. The technologies for virtual consultations that took the commercial provider Babylon years to establish in two cities have become established across general practice in weeks. General practitioners are beginning to look like doctors working in a salaried service, instead of being sub-contractors. There is growing interest in a salaried option, especially among younger GPs5. Here there has been a growing sense in general practice that it could not go on in its present form, and NHS England agreed, although it did not anticipate a sudden change.
- Spare capacity and labour direction Not only has the NHS taken up direction of professional labour, encouraging forward movement of specialists into A&E departments and seconding nurses to work in field hospitals, but it is also mobilising ‘returners’ from among the recently retired. Volunteers have also come forward in large numbers to provide temporary support for isolated people staying at home without family support. Managers in the NHS will want new, flexible ways of working to remain but some professionals may want to return to the status quo ante; both camps will search for political alliances.
New capacity was created by conversion of existing premises into infectious disease wards with ventilation capacity, and by construction of large field hospitals like the 4,000-bed Nightingale Hospital in London. The NHS bought almost all spare capacity (in terms of beds and staff) in the commercial medical sector. These acquisitions may not be permanent but there will be a backlog of postponed surgery and cancer treatments to work through, and spare capacity in theatres and beds will help this. The need for slack in the system has been acknowledged for a decade but now there is publically visible spare capacity which may prove difficult for politicians to close.
- Integrated health & social care By contrast, the NHS has failed, despite decades of talking, to reach agreement with local government social services, and so is still handicapped in transfers of mostly older people with multiple problems out of hospitals into community settings. Retired social workers are not being called back into action.
This historic mismatch may yet change, but it will probably do so slowly. There are accounts of some Integrated Care Organisations (which depend on collaboration between local government and the NHS) developing quickly because managers who would often act as brakes to progress are absent, dealing with Covid-19 planning. Others report that the NHS and local government operate with same distrust and disregard for each other as usual.
This is a deeply entrenched problem that successive governments have promised to uproot, but nothing much has happened. One suggestion that may offer employment opportunities during the coming recession is the formation of a community health worker service staffed by young people who have gone through a crash training programme6. And smaller changes may also make a difference. How different the NHS response to Covid-19 might have been if Advance Care Plans were in place for vulnerable older people like those living in care homes. Such plans should contain the option for us to decline ventilation, just as we may decline resuscitation. The NHS knows what to do but government has prevented change; it will probably work around the problem, but avoid trying to solve it
- Market mechanisms The government has abolished payment by results and payment by performance in the NHS, and suspended payments for target achievement in general practice. It has also written off the debts that hospital and community trusts have run up with the Department of Health, a “hair cut” that has been talked about for two years. These are blows to the marketisation of the NHS, and will re-inforce the existing enthusiasm for direct control of the NHS from the centre. The NHS is beginning to look like a service that is clinically-led rather than target-driven. The supply failures suggest that it is time for the NHS to grow its own PPE and diagnostic testing kit manufacturers, in-house. A long-standing policy of marketisation may well be rolled back further when the full benefits of command and control management become evident
- Public engagement & case mix Constant encouragement to relieve pressure on the NHS seems to have had an effect; attendances at A&E departments fell by one third in March 2020, the biggest fall being among young adults. With hospitals being depicted as dangerous, infectious places, potential A&E users are understandably avoiding them. Supplier-induced demand may also be reduced, as doctors and nurses prioritise those with infections and pay less attention to others, reducing follow-up or onward referral to outpatient clinics of patients who do not have Covid-19. Use of health services (often confused with ‘demand’) has risen relentlessly, but Covid-19 has stopped this. The public will want normal services to resume. There may be a latent desire to change but not the capacity; Covid-19 is a disruptor that causes an emergency mobilization but not long-term changes in behaviour.
These are only the most salient of examples of possible long-term changes in the NHS being initiated by short-term responses to Covid-19. Not all changes will take root. But overall the old order of the NHS will be shaken.
This blog is an expanded version of ‘The NHS takes control’, published in Renewal – a journal of social democracy 2020;28(2):15-19
Sources:
- Matthew Taylor How the coronavirus crisis could change the nature of government and democracy The Policy Institute, Kings College London. 3rd April 2020
- Sarah Dalglish Covid-19 gives the lie to global health expertise The Lancet March 26th 2020
- The lockdown and the long haul, The Economist 21st March 2020
- Joe Buckley & colleagues A science-based socialist response to Covid-19 Scientists for Labour March 2020
- Jacqui Thornton How coronavirus will change the face of general practice forever BMJ 2020;369: m1279
- Andy Haines and colleagues, National UK programme of community health workers for Covid-19 response. The Lancet March 24th 2020
So why is a GP publishing about Covid radiology?
By Nathan Davies, on 31 July 2020
By Melvyn Jones
I have just co authored a BMJ piece on chest radiographs with Covid pneumonia – The role of chest radiography in confirming covid-19 pneumonia So why is a GP publishing about Covid radiology? 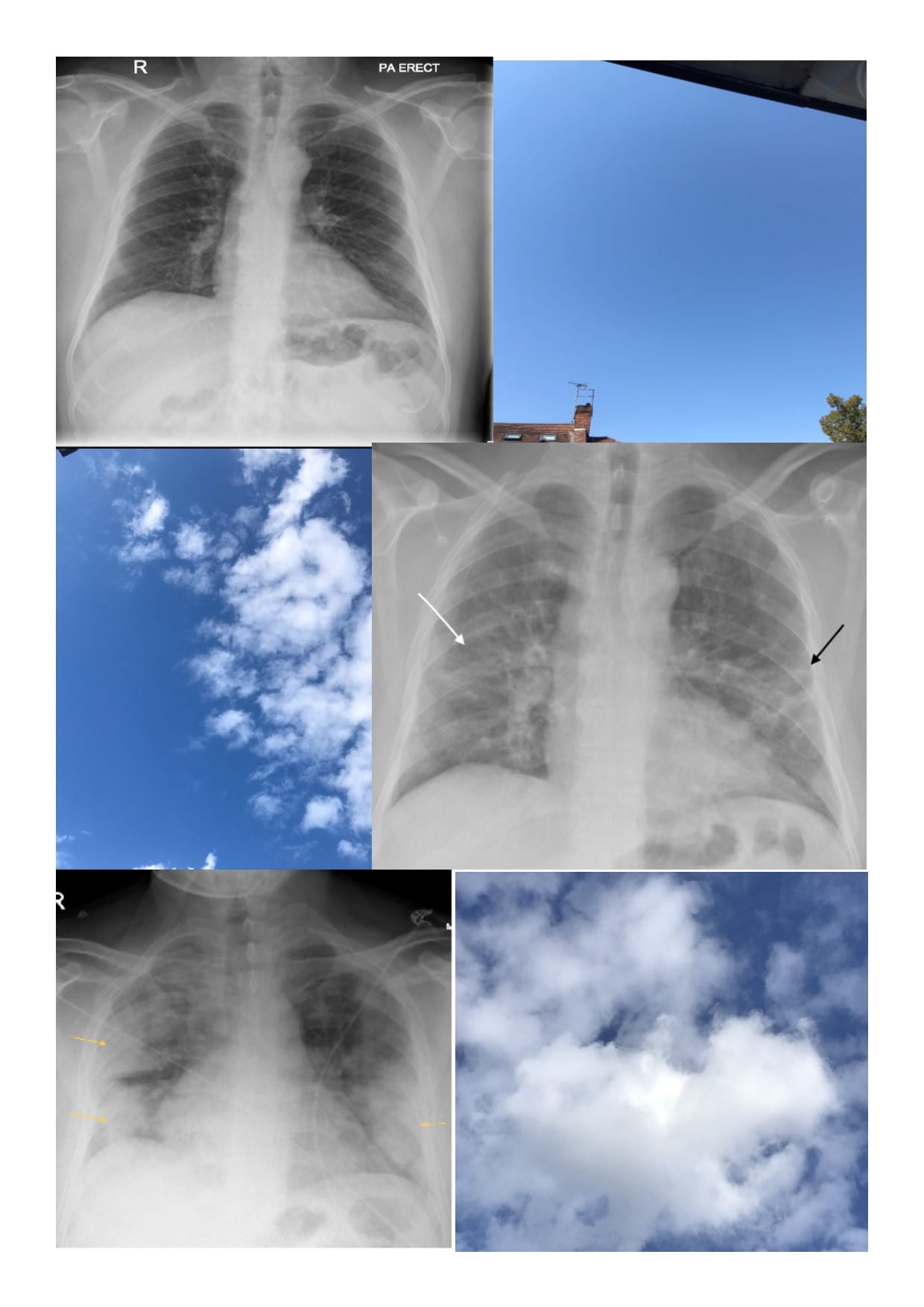
My wife is a radiologist with a special interest in chest radiology and a love of a good chest x-ray; back in March she was starting to see the x-rays of the first patients with covid pneumonia and she was shocked. She hadn’t ever seen x-rays like this. This was something really different.
There were real fears that hospitals would be overwhelmed and we knew clinicians who never normally look at a chest x-ray anymore were being marshalled in to support the covid response. Would they know what to look for on the chest x-ray? Could we do something to help? So I wrote to the BMJ pitching an idea on the 22nd March. They liked the idea and commissioned us to do a “Practice pointer”, not a traditional systematic review but an article based on evidence and clinical experience. I interviewed my wife to capture the key points and while she was on call went searching for good images. My literature search revealed 20 articles and only 1 related to Chest x-rays, there really wasn’t much out there. We had our submission ready and posted it on the 30th March and by that stage 1200 UK patients had died of Covid.
I needed to understand a bit of radiology to work though the literature. What is ground glass opacification (“the lung markings are still visible through the Covid changes”) and how it is different to consolidation- key concepts with Covid pneumonia. Covid lockdown meant the possibility of eating breakfast outside and thinking things through in a slightly less pressured environment. Should I admit to looking at the cloud formations during those few weeks of glorious weather? I did, I do. Cirrus clouds were my ground glass, I could still see the sky through these light feathery clouds, cumulonimbus was my consolidation; thick, opaque and ominous.
There then followed 6 revisions and further major changes requested by the team that ready it for publication. It went out to 7 different peer reviewers; many of whom made valuable but conflicting requests for changes but the overwhelming message was – this needs to be out there, now. We also needed input from a physician who was in the thick of it- how were they actually using imaging as part of their assessments of breathless Covid patient? I was working with James Piper – an Acute Medicine doctor at the Royal Free as part of the MB BS teaching programme and he was happy to help.
We turned round each iteration within 48-72 hours but still the requests for changes came. The numbers of UK deaths went relentlessly up. Eventually it was accepted, type set and finally published on the 16th July. UK deaths had now exceeded 45,000, Google scholar had hundreds of Covid articles and we were coming out of lockdown. It was a pleasure to see it finally published but there was a real sense that it was just too late. That’s the thing with the BMJ though; the day it was published it was downloaded over a 1000 times, two weeks later it has been viewed over 7000 times. The really helpful thing though for someone who is not a big user of social media, was seeing who Tweeted about it and where. The BMJ link had been re-tweeted 147 times and to places like South Africa, South America and India- all parts of the world which were now facing their 1st waves of this terrible disease and today the newspaper headline is “Europe faces its 2nd peak”. It may be of use to a clinician somewhere having to manage yet another patient with this awful disease, so may be we could and did do something?
Supporting carers of someone living with dementia during the coronavirus pandemic
By Nathan Davies, on 28 July 2020
In this post Dr Kirsten Moore, Marie Curie Palliative Care Research Department, UCL talks about dementia and supporting those living with demenita during the coronavirus pandemic. 
Who is dying with Covid-19?
In April this year Covid-19 (coronavirus) became the most common cause of death in the UK. Office for National Statistics data showed that most deaths caused by the virus in England and Wales were among older people and those with underlying health conditions.
One fifth of people dying with coronavirus had dementia, making it the most common pre-existing condition. Also, the death rate from dementia was significantly higher in April than the previous five-year average.
How is COVID-19 impacting family and carers?
In the UK 700,000 family members and friends support someone living with dementia, providing 44% of the cost of care for people living with dementia1. Being a carer can negatively impact finances, stress and physical and emotional health. In our recent publication we highlight some of the end of life care challenges that coronavirus has created for families caring for a frail older person or someone with dementia.
A diagnosis of dementia often leads to reduced social interaction for both the person with dementia and their family carer. Social distancing and lockdown measures are increasing this isolation and loneliness. Carers may have additional worries supporting the person with dementia who may not understand the importance of shielding and keeping socially distant from others.
End of life discussions and planning
When a person with dementia lacks capacity to make decisions, families may be faced with difficult decisions about whether to send their relative with dementia to hospital or a care home for care, or whether to provide end of life care at home where they can be present with their relative. Alternatively, they may have these decisions taken out of their hands due to procedures and guidelines adopted to contain the spread and impact of coronavirus.
In advanced dementia communication may be limited for many months. Having discussions in the early stages of dementia gives someone with the condition an opportunity to express their preferences about end of life care.
There are many benefits to discussing our end of life wishes with our family and those who are important to us. They allow us to share how we want to be cared for and who we want involved in decision making if we can no longer make or communicate decisions.
These discussions can also help family feel more confident in making decisions if the person living with dementia lacks capacity. When family members are unsure what a person wanted at the end of life, they may worry they have made the wrong decisions or feel guilty if the person had an uncomfortable death.
However, these conversations are not easy. Discussing end of life is something most of us tend to avoid. It is difficult to face our own mortality. These conversations are also difficult because we don’t know what is likely to happen or what sort of decisions we, or our families, may be faced with. Often discussions tend to focus on resuscitation status, place of death or whether someone should be taken to hospital.
People who have dementia may find it difficult to imagine situations that they have not yet faced, such as difficulties swallowing and talking.
How can we support carers?
Simply keeping family carers involved and informed is an important way healthcare professionals, hospitals and care homes can support family carers. This may involve having conversations about place of care and end of life care.
There are numerous guides about difficult conversations, such as this Marie Curie blog. There is no one-size-fits-all approach, but the most difficult part is often starting the conversation. Healthcare professionals may be worried about raising end of life topics, that they may not have all the answers or that the family may not want to have these discussions. Carers, however, usually prefer an open and honest conversation, including being told that there may be uncertainty or no clear answers.
Being responsive to whether the carer is ready to have a conversation is important. There may be a pressing need for a conversation, but if discussions are raised at an earlier point in the dementia trajectory then it can give the carer more time to prepare themselves for discussing end of life.
What can carers do?
Family and carers may feel that if a conversation about end of life is needed, it will be raised by healthcare professionals. However, this may not always happen. Carers should feel reassured that if they have questions about the care of their friend or relative, that they should feel able to ask healthcare professionals for information and advice.
You may find it helpful to talk decisions out loud or write down a list of pros and cons. These simple strategies can help you clarify what is important or where you need more information or advice. It is important to get information from reliable and trusted sources. Make use of helplines such as the Marie Curie, Dementia UK or Alzheimer’s Society helplines.
Having a family member who understands how dementia progresses has been linked to a more comfortable death for care home residents. Keep in mind the best interests of the person with dementia if they lack capacity to make their own decisions. Think about their values and what would be important to them. It may not be realistic to follow all their wishes, so do not feel guilty if this cannot be achieved.
Developing a decision aid
To help guide families and carers in making some of the complex and challenging decisions raised here, our team at the Marie Curie Palliative Care Research Department at University College London are developing a decision aid.
We will be exploring the questions that people are asking Marie Curie and the Alzheimer’s Society to work out the biggest challenges facing people with dementia and their families during the pandemic.
We will then work with family carers, healthcare professionals and use existing research to develop a decision aid. The decision aid will help carers think about their current circumstances and provide relevant information to help inform their decision making.
Sources
1. Prince, M., Knapp, M., et.al. (2014). Dementia UK Update (2nd edition).
This blog was originally posted on the Marie Curie website, taken with permission from Marie Curie and Kirsten Moore. https://www.mariecurie.org.uk/blog/supporting-carers-dementia/277479
Signposting patients to sexual health online – don’t forget the health (or the sex)
By Nathan Davies, on 22 May 2020
In this post Julia Bailey discusses the impact of Covid-19 on sexual health services and discusses sexual health online.
The Covid-19 pandemic has prompted an unprecedented shift to remote health services as a response to social distancing for patient and practitioner safety. Sexual health clinic capacity has been cut as staff have been deployed to other parts of the health service, and patients are now asked to contact health services by phone or vi deo-link, with clinic visits reserved for a small proportion of people who need to be seen (FSRH guidance). People can also access online sexual health services for STI testing (+/- contraception), in areas where this service is provided.
deo-link, with clinic visits reserved for a small proportion of people who need to be seen (FSRH guidance). People can also access online sexual health services for STI testing (+/- contraception), in areas where this service is provided.
The shift to remote consultations is likely to make it more difficult to offer holistic healthcare and health promotion. For example, patients welcome opportunities to discuss sexual wellbeing beyond physical health (e.g. sexuality, sexual difficulties, sexual pleasure), but picking up on this will be more challenging with less opportunity to notice non-verbal cues and to establish trust (e.g. whilst examining).
Resources via the Internet and mobile phone can offer private, convenient access to information, which may be particularly welcome for topics which can be difficult to discuss (e.g. sex, sexuality, sexual difficulties). Online sexual health services can offer efficient STI testing and treatment, but do not usually offer evidence-based sexual health promotion. Interactive (i.e. tailored) digital interventions are effective for learning and sexual behaviour change, and could be incorporated into online sexual health pathways.
There is no nationally commissioned digital sexual health programme, and digital innovation varies widely across the UK. There are thousands of health apps and websites, but only a tiny minority have been rigorously evaluated and it is difficult to know which to recommend – the NHS apps library curates trustworthy resources.
Digital sexual health resources for patients – some suggestions:
Before (or instead of) appointments:
- Covid-19: Accessing sexual health services
- Websites for young people: e.g. Brook, BISH, SexEtc
- Online information and advice: Sex and sexuality; Relationships; Contraception; STIs and HIV; NHS sexual health information
- Symptom checker: NHS 111 Online; Patient Info
- Decision aids (e.g. Contraception choices; Hormone replacement therapy)
- Videos prior to appointments (e.g. Implant insertion and removal; IUD/IUS insertion; Cervical smear procedures)
- Mobile phone apps e.g. for sex and pleasure, alcohol harm reduction, smoking cessation.
- Interactive digital interventions e.g. for condom use; STI/HIV prevention; sexual difficulties
After a diagnosis/ongoing support:
- Trustworthy patient information (e.g. herpes; genital warts; Hepatitis B, Hepatitis C; HIV)
- Electronic partner notification
- Text message interventions: g. for safer sex, STI testing; support after acute STI diagnosis
- Online support groups (e.g. HIV support; + Support Groups; Health Unlocked forum)
- Email or text reminders (e.g. for contraception or HIV medication including PrEP)
Tips for writing patient materials
- Don’t reinvent the wheel! Check what’s already available
- Involve target users to make sure material meet their needs, priorities and preferences
- Draw on principles of evidence-based sexual health promotion
- Address barriers to access, e.g. audio and video formats; material in first languages
- Address groups whose needs are often overlooked (e.g. women who have sex with women, trans, non-binary, intersex, and disabled people).
Summary
The post-pandemic ‘new normal’ will include digital health. There are some excellent online sexual health information resources available, and there is currently an unprecedented opportunity to offer evidence-based, tailored sexual health promotion to complement online and clinician-delivered sexual health services.
(This post was originally posted on the BMJ Sexual and Reproductive Health website who have provided permission to repost)
Families struggle to know what’s best for older relatives with dementia during COVID-19
By Nathan Davies, on 22 May 2020
This post is a press release from Marie Curie about the latest Covid-19 work being led by Dr Nathan Davies from our Centre for Ageing Population Studies.
about the latest Covid-19 work being led by Dr Nathan Davies from our Centre for Ageing Population Studies.
Families need more help to make quick decisions about the care their dying older relatives with dementia should receive during COVID-19, say UCL researchers, with the support of Marie Curie and the Alzheimer’s Society.
Many older people with COVID-19 will have dementia which affects 22% of people aged 85 and over1. They may experience a sudden deterioration with rapid onset of respiratory failure. Given the high death rates from COVID-19 in older people, even in hospitals, it is hard for people with dementia and their families to know what the best thing is to do about treatment and care options.
For those who lack the ability to make decisions for themselves, it may also mean that families have to make very quick decisions under stressful circumstances, for instance about resuscitation. They will also have to weigh up the pros and cons of either sending their elderly relatives to hospital for medical attention or receiving palliative care at home, where they may be more comfortable, and families will be able to maintain contact with them.
Having to make these difficult decisions can have a profound impact on the emotional well-being of family members, and lasting feelings of guilt and doubt if they made the right decision.
Researchers from the Marie Curie Palliative Care Research Department and Centre for Ageing Population Studies at UCL are producing an evidence-based guide, for family carers and people with dementia to use in the management of COVID-19. It is estimated that nearly half a million people with dementia in the UK live in their own homes2. Latest available data also shows that 38% of all COVID-19 deaths occur in people aged 85 and over (up to 24 April)3.
The research team hopes that the new guide will also ease the emotional burden that families can experience and help resolve any feelings of uncertainty about the decisions they have made for their loved ones.
Tracey Lancaster, whose mum is living with dementia said: “I’m dreading the call from the care home to say that mum has coronavirus. I worry about her fighting for breath and therefore we would have to decide if she goes into hospital or what care can be provided in the home. I’m not sure that I could make that decision. So, a decision guide like this one would be invaluable for me and my family.”
The rapid project, funded by an Economic and Social Research Council COVID grant and supported by end of life care charity Marie Curie and Alzheimer’s Society, will identify factors influencing place of care and death in older people as well as the key challenges and decisions which family carers of people living with dementia are facing currently in the COVID-19 pandemic.
The pandemic brings extra challenges to those who are ‘social distancing’ from their older relatives – and means that they may also need to make quick decisions over the phone with a professional they’ve never met.
Co-lead researcher Dr Nuriye Kupeli, Senior Research Fellow at Marie Curie Palliative Care Research Department, UCL Division of Psychiatry and an Alzheimer’s Society Fellow, said: “It is a difficult time for people living with dementia and their carers. Due to measures such as social distancing, self-isolation and shielding, people living with dementia and their carers may not have access to support and guidance when making difficult decisions. This work will help us to understand better how people living with dementia and their families are managing important decisions about care during COVID-19 and how best to support them.”
Co-lead researcher Dr Nathan Davies, Senior Research Fellow at Centre for Ageing Population Studies, UCL Institute Epidemiology and Health, and Alzheimer’s Society Fellow, said: “This is such an important project and follows on work we’re doing prior to COVID-19. Many families caring for someone living with dementia will be making daily decisions on behalf of their relative with dementia. But we know many will not have discussed or planned end of life care.
“The nature of COVID-19, which can worsen rapidly, means they will be forced to make quick decisions with potentially little support or information. They may be feeling overwhelmed considering what is best for their relative. The decisions they make may have a lasting impact on their grief and wellbeing: We want to try and help support carers with decisions to ease these feelings.”
The researchers say that having early and open conversations about end of life wishes with older relatives, particularly during COVID-19, could avoid potentially futile and burdensome interventions at the end of life while ensuring that loved ones get the compassionate care they need.
Marilyn Beattie, whose husband Gordon died in 2019, following a dementia diagnosis, said: “I felt like I was shooting in the dark most of the time. I didn’t know who to turn to, or what was available. It would have changed everything if I had an aid like this – a life-changer.”
Matthew Reed, Chief Executive of Marie Curie said: “At Marie Curie, we understand the value of planning ahead for the death of a loved one. However, when this isn’t possible, particularly during these uncertain times, it’s important that families living with dementia are properly supported to make difficult decisions and are not left with a legacy of grief and guilt because they’re not sure they made the right choice in a moment of crisis.”
Fiona Carragher, Director of Research and Influencing at Alzheimer’s Society said:
“Alzheimer’s Society are proud to unite with Marie Curie to support this urgently needed research. Covid-19 has severely affected people with dementia and their carers, and our Dementia Connect support line has been flooded with thousands of calls for help. This new, evidence-based guide will help carers and people living with dementia feel informed and supported, practically and emotionally, when making important decisions about care during the pandemic including hospitalisation, treatment and Do Not Attempt CPR.
“We know that the current crisis is making choices like these even more difficult which is why it’s so important Alzheimer’s Society researchers use their expertise to support people through this.”
Dementia research behind the Scenes: Experience of an A-level student in an academic department
By Nathan Davies, on 27 September 2019

Vennie working with Nathan Davies learning about our dementia projects
We have a fantastic post below from Vennie an A-level student aspiring to study Medicine at university. She visited the department and shadowed some of our academics in their various projects in July. In this post talks about her experience and what she took away from it.
Dementia is an increasing problem especially with the growing older population in the UK. The awareness of dementia is rising, especially through the use of media and organised events such as Memory Walks. However, how much do we know about dementia?
Well, in simple words, dementia is the ongoing decline in the brain. This is only an umbrella term for 200+ different sub-types of dementia that exists, some of which you may have heard off. For example the most common two are Alzheimer’s disease and vascular dementia.
During my placement in the Research Department of Primary Care and Population Health at the Royal Free Hospital, I was able to shadow members of the team that are involved at different levels of research projects.
I discovered that there are many stages which make up the process of a research project. Starting with the planning and design of the research project, ethics, and recruitment through to finally analysing and presenting the results produced. Alongside all this and integrated throughout are processes to ensure the results are implemented into clinical practice and policy, to make a difference. I learnt about the different types of studies such as qualitative studies and large clinical trials. Due to the involvement of human participants including often patients from the NHS in the studies the department runs, a major part of the research process is the ethical application and review. The purpose of the review is to establish if the project has more benefit than risk to the person and their family as well as is the project being conducted sensitively. For all of this to happen, it may take 5 to 20 years to see a difference in practice and policy.
In order for, this project to be successful, a range of people are required to take part, which in turns bring a variety of skills into the mix. These individuals may include designers, programmers, clinicians, psychologists, sociologists, statisticians, qualitative researchers, and importantly patients and their family themselves. A few of the most prominent skills are communication, teamwork, determination and resilience. For example, a project with Dr Davies and Prof Rait I observed on producing a support package for people with dementia and their families, communication has a massive role to play. The project uses workshops with people with dementia, their family and professionals to develop the support package. There is a need for clear communication between the ranges of people for this project to progress smoothly. The communication may come in the form of discussion-based in meetings, emails and many other ways. Therefore, teamwork is essential as each person will have a special role in the project. Finally, determination and resilience are required from every member of the team as there will be challenges along the way, which could be out of your control that must be overcome. For example, if the project does not meet the criteria of the ethics committee it may be returned to the researcher, and his or her team must go back and amend the plan.
In conclusion, research of any kind similar to this project requires a range of people to be involved with a variety of skills that are vital for the research to work. This work experience has been a fascinating and exciting opportunity for me to experience what goes on behind the scenes of a research project.