 Close
Close

“The patient bore the operation with great fortitude” – Lochland Shiel’s facial exostosis
By H Dominic W Stiles, on 28 April 2017
In Guy’s Hospital Reports for September 1836, there is an article, “Cases of exostosis of the bones of the face, disease of the cranium, and fractures of the frontal and parietal bones requiring operation, by Mr. Morgan.” Mr. John Morgan was a pupil of Sir Astley Cooper. Plarr’s lives of the Fellows, tells us that Morgan “showed an intense interest in natural history, and began to stuff birds and small animals almost as soon as he could use a knife and his fingers.” We also discover there, that he dissected an elephant named ‘Chum,’ took an awful lot of snuff, and was one of the founders of the Zoological Gardens in Regent’s Park, now London Zoo. His brother-in-law William Gosse who was a surgeon and was related to Philip Henry Gosse, emigrated to Australia.
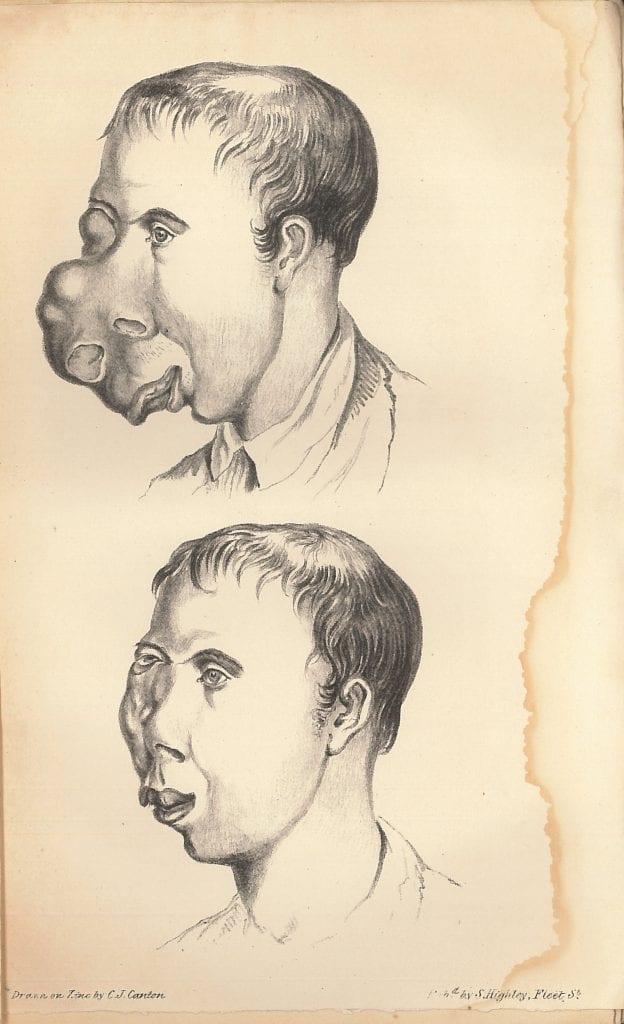
The case we are looking at, Case 1. Exostosis of the Bones of the of the Face, (the notes taken by Mr. Collin), covers an unfortunate Irish labourer, Lochland Shiel, admitted on the 1st of August, 1835 (Guy’s Hospital Reports, p.403-6). At the time he was 24 years of age. Shiel told the doctors that until he was fifteen he had good health, when he noted a small tumor in his right nostril. He was told by ‘a medical man’ that it was ‘of no consequence.’ However, as we can see in the plate, after nine years it had grown greatly, distorting his face,
the right nostril being enormously expanded and closed by the enlargement of the tumor, which, from its size, completely concealed the eye on that side, and extended downwards into the mouth, being there connected with the palatine and alveolar processes of the right superior maxillary bone; projecting also forwards, so as to press the lip beyond the teeth, to the extent of two inches. The bones apparently implicated in the disease were the ossa nasi, superior maxillary bone, vomer, and the inferior turbinated and malar bones.
[…]
The poor fellow, when admitted, complained of no pain; and I could not find that his sufferings had given him much inconvenience, during the whole of his disease.The general health appeared good; but he was greatly emaciated, more, I believe, from want of proper food, than from the constitutional effects of his disorder.
Deciding that the tumor was common exostosis, an opinion in which Morgan was supported by Sir Astley Cooper and Dr. Hodgkin, he “removed the morbid excrescence” on the 6th of November. He first made an incision over the right nostril, to ascertain that it was indeed exostosis.
A semilunar incision was then made, extending over the nostril, from the internal angle of the right eye to the centre of the the upper lip. A similar incision was made on the outer side, commencing at the angle of the eye, and joining with the other, at the lip. The integuments were then dissected from around the tumor, , and a metacarpal saw was used for its removal; and as it was of a spongy texture, it offered little resistance to the instrument. No great quantity of blood was lost during the operation , the exostosis not being very vascular; and it was only found necessary to secure one vessel, a superficial branch of the transverse facial. all further disposition to haemorrhage was easily restrained by pressure.
After the tumor had been thus removed, the integuments were brought together by an uninterrupted suture; a dossil of lint was placed over the wound, and confined by adhesive plaster; and over all, a light bread-and-water poultice was applied.
The patient bore the operation with great fortitude; and said afterwards, that he suffered but little pain, excepting when the first incision was made.
[…]
Up to the the present time, the patient has been going on well; all discharge from the face has almost entirely ceased: hardly any exfoliation of bone has taken place; his general health is restored. The present appearance of his face is correctly represented in the accompanying plate. (Guy’s Hospital Reports, 1836)
Unfortunately I cannot locate any record of Lochland Shiel on family history records or census returns, though a Locklin Sheels married a Margaret Boyle in Newcastle-under-Lyme on the 22nd of December, 1834. That might be him. It could be that he was missed, it could be he spent time in Ireland, or it could be that his name has been wrongly transcribed. If you have any ideas about where in Ireland he was from, or any family, do contribute in the comments. In the spring of 1842 Shiel died in Birmingham.
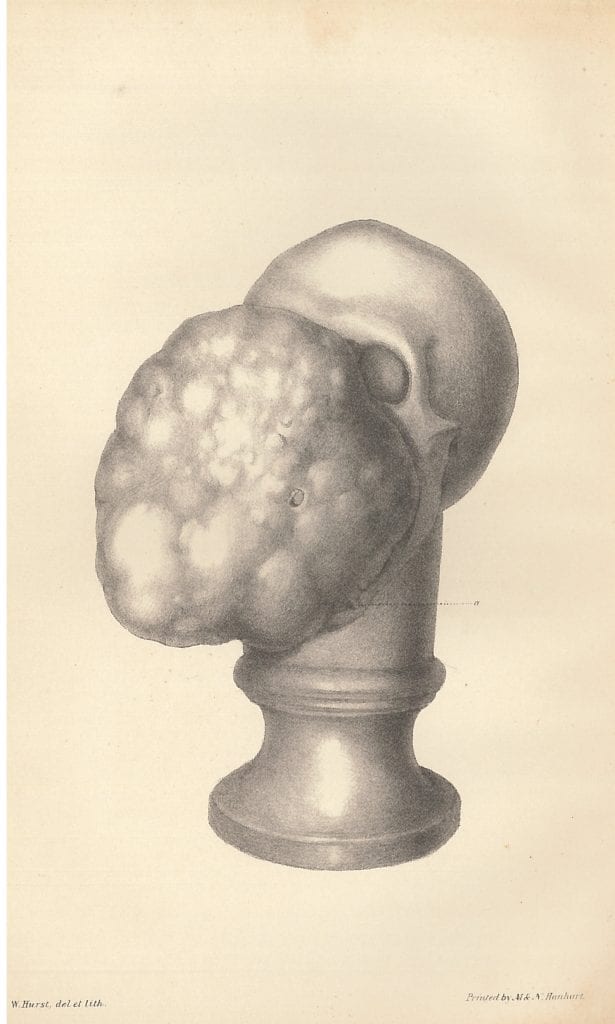
We have been unable to learn the particulars of the termination of the case. It may, however, be observed, that his death did not take place til nearly seven years after the operation; so it may fairly be said to have been prolonged by it for nearly that period. It is, however, impossible to look at the cast taken after death without marvelling that life could have been prolonged to such a period. The growth appears to have been simply enormous — larger indeed than the head itself. (Guy’s Hospital Reports, 1842)
I have been unable to find a death record for anyone of his name. Someone must have dissected his remains to make a cast of the tumor – and presumably, his skull. Below is the cast that shows the tumor. As you can see, it had grown enormously in the following years. The dotted line points to the tiny space through which Shiel ingested food.
 Guy’s Hospital Reports, No 2, September 1836 p. 403-6
Guy’s Hospital Reports, No 2, September 1836 p. 403-6
Guy’s Hospital Reports, No 15, October 1842 p. 491
A System of surgery v. 3, 1882, p.259
[minor updates 15/10.2018]