 Close
Close

Thinking about how we support family carers of people with dementia in light of carers week
By guest blogger, on 10 June 2021
In this post Nathan Davies talks about some of the recent work he has led on support family carers of people living with dementia, and talks about some of the Covid-19 work which has been implemented in the NHS.
This week marks Carers Week, you may have all seen in the media the wealth of stories and people talking about the challenges that informal carers (friends or family) have experienced over this past year during the pandemic. Carers UK have reported this week that 72% of carers have not had any breaks from their caring role since the start of the pandemic (1).
We know one of the most demanding caring roles is caring for someone living with dementia, with over 750,000 carers currently in the UK. Most of my work looks at how we can support family carers, in particular in the later stages of dementia or planning for the end of life. This is a particularly difficult time for carers and one of the key challenges they face is making decisions about the individual’s care. Decisions may include moving into a care home, increasing the amount of support, managing eating and drinking difficulties, and ensuring the everyday well-being of the individual.
In a recent project we explored the decision-making process carers go through and how they make decisions(2). We developed a model of decision making which considers the context and the processes involved. Making this process and the context explicit may be helpful for carers as a guide to help their thinking when making complex decisions, but also for professionals when trying to start significant conversations.
It is important to consider the context in which decisions are being made including the individual’s personal preferences about their care, any advance care plans they have made or lasting power of attorney in place, considering if the person still has capacity and what their current health status is, and finally, thinking about what support is available from others.
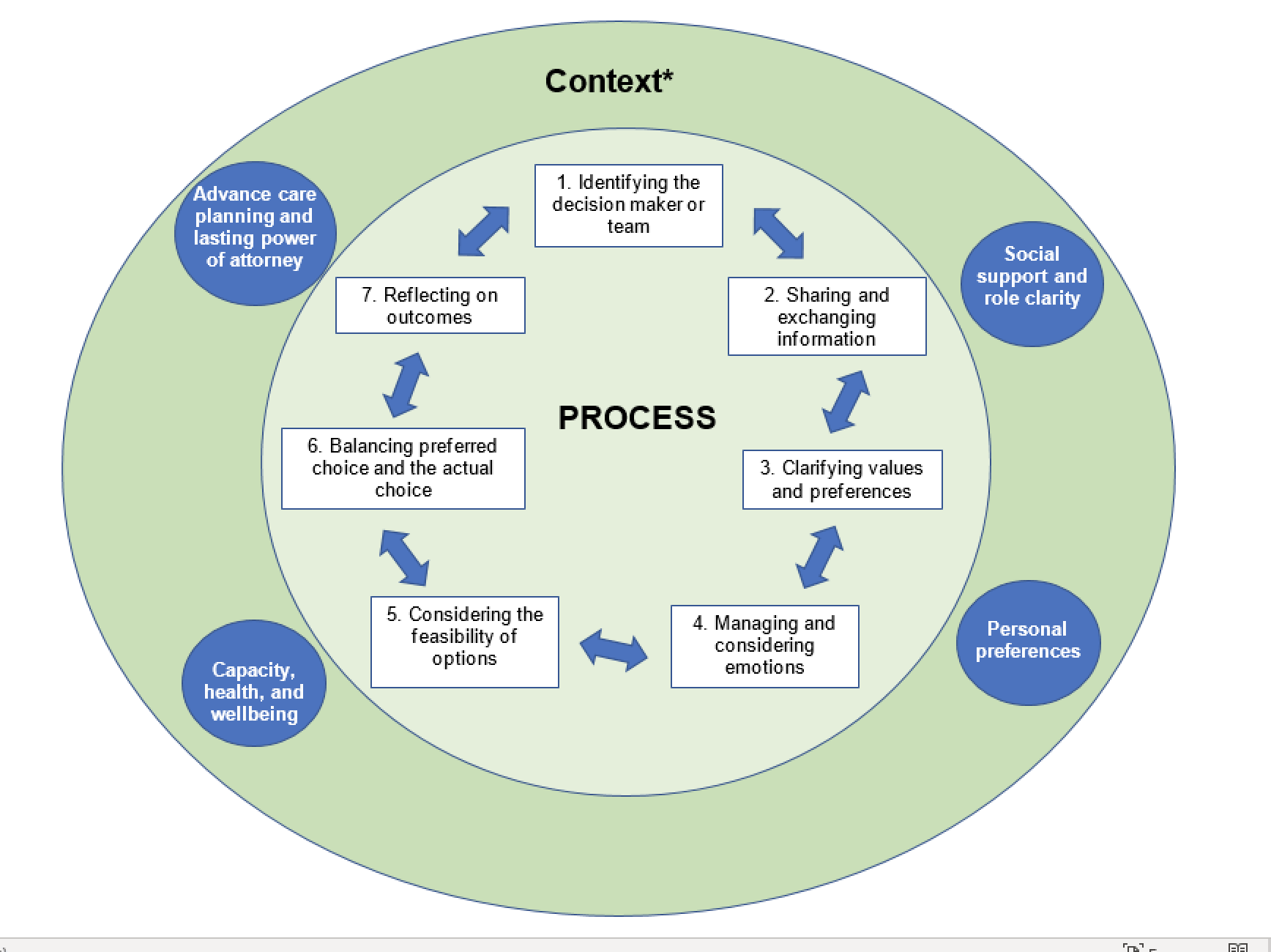
As you can see in the image there were 7 stages in making a decision:
- Identifying who is the decision maker or the team and clarifying what is their role
- Sharing information about the decision which needs to be made, this may include what the problem is, what are your options etc
- Clarifying what is important to those involved, considering their values and preferences, being mindful of disagreement
- Managing and considering the emotions involved in making what can be quite significant decisions
- Think about what is the feasibility of the options which are available – this is likely to include finances and the impact on the wider family or support network
- Balancing what you would like to do (preferred choice) with what you can actually do
- Make the decision and reflect on the outcome of this decision to inform further decisions or refine your decision
Now this may all seem rather theoretical, but we have already used this to create some applied resources which carers and professionals can use to help with discussions and decisions.
We have developed a decision aid to support family carers of people living with dementia who are at risk of or who have Covid-19 and are not able to make their own decisions. The decisions focus on care at home, care in the care home and care in hospital. In particular, we have included:
- How to manage care at home
- How to support your relative/friend in a care home
- What to do if they become unwell
- Should they go to hospital
- How to keep in touch if you can’t visit
We provide a variety of information including the signs and symptoms of COVID-19 which may be different for older people, and the legal aspects of making decisions. We bust some myths about what support options are available at home. We also consider the benefits and advantages of different options of care including going into hospital.
This guide has been widely shared and is freely available online. It has been implemented as part of NHS England and NHS Improvement Dementia COVID-19 Pathway.
The latest version of the decision guide is available now from: https://www.ucl.ac.uk/psychiatry/decision-guide
For our work on this we also won Alzheimer’s Society’s Dementia Hero Award for Research.

- Carers Week 2021 report. Breaks or breakdown Carers Week 2021 report. London; 2021.
- Davies N, De Souza T, Rait G, Meehan J, Sampson EL. Developing an applied model for making decisions towards the end of life about care for someone with dementia. PLoS ONE. 2021.
Health messaging to encourage key protective behaviours to reduce the spread of Covid-19: What we can learn from existing evidence about getting the message right?
By guest blogger, on 18 May 2021
In this months post Dr Sadie Lawes-Wickwar, a Health Psychologist and Lecturer in the department teamed up with other health researchers, health psychologists, public health practitioners, and public contributors across the UK during the COVID-19 pandemic to find out what we can learn about getting the message right to support the public to prevent the spread of Covid-19.
In the event of an outbreak of an infectious disease, the population is required to make often rapid changes to their behaviour to reduce the spread. Public health campaigns can support population-level behaviour change, but it is crucial that the public receives consistent, clear information, so they understand what it is they need to do new (e.g. when using fa
ce coverings). However, public information during a pandemic can be conflicting, change frequently, or use language that the general population may find it hard to understand. We need to think
carefully about the messages that are used to instruct the public to perform behaviours that are key to reducing the spread of a virus.
After the outbreak of Covid-19 in the UK last year, a collaborative group of health psychologists, behavioural scientists, public health practitioners, and members of the public formed the Health Psychology Exchange to support the public health response to the pandemic. A group of Health Psychology Exchange members set about reviewing existing evidence to inform recommendations for local and national public health teams in developing health campaigns. Our aim was to identify what characterises effective public health messages for managing risk and preventing infectious disease, and what influences people’s responses to such messages.
Our first review of public health messaging found that, to influence behaviour effectively at the population level, messages need to be acceptable to the populations they are targeting, be delivered by credible and trustworthy sources, and in language target populations can understand, to increase understanding and threat perceptions [1]. Specifically, in the context of encouraging vaccine uptake, evidence tells us that providing information about virus risks, vaccination safety, vaccine clinics, and addressing misunderstandings about vaccines, can support uptake at hospitals (e.g. among hospital staff) or within local communities. We can also support understanding and beliefs about vaccines by framing messages in a particular way, such as emphasising the reduction of risks and the benefits to society from being vaccinated [2].
Our work has highlighted gaps in research and the development of previous public health messages, including the valuable input of the public in the design, delivery, dissemination and evaluation of health messages [2]. One of our key recommendations has been the involvement of local communities in all aspects of the messaging process, which is also in line with recommendations from the World Health Organisation (WHO)[3]. We also need more high-quality research to demonstrate the effects of messaging interventions on the uptake of recommended behaviours. Surprisingly few studies to date have evaluated messages adequately to be able to conclude the definitive impact of campaigns on population-level behaviour, such as vaccine uptake.
Our recommendations have informed two British Psychological Society (BPS) Behavioural Science Disease Prevention Taskforce guidance documents to date, one to support public health teams to deliver effective public health campaigns, and another to optimise vaccination uptake during Covid-19. Using behavioural science can boost public health campaigns during the Covid-19 pandemic, and I hope to see more collaborations between health psychologists and public health teams in the coming months as we look to a brighter future.
- Ghio, D., et al., What Influences People’s Responses To Public Health Messages For Managing Risks And Preventing Disease During Public Health Crises? A Rapid Review Of The Evidence And Recommendations. PsyArXiv Preprints, 2020.
- Lawes-Wickwar, S., et al., A rapid systematic review of public responses to health messages encouraging vaccination against infectious diseases in a pandemic or epidemic. Vaccines, 2021. 9(2): p. 72.
- WHO, Communicating risk in public health emergencies: a WHO guideline for emergency risk communication (ERC) policy and practice. 2017: World Health Organization.
What can students do to make the most out of their Master’s degree?
By e.schaessens, on 8 July 2020
By Louisa Manby and Kirsi Sumray
We are both students on the Population Health Masters programme at UCL. Louisa came to UCL after undertaking a BSc in Biomedical Sciences at The University of Manchester. Kirsi completed a BA in Anthropology at The University of Bristol in 2017, took a gap year and then worked for the British Red Cross before returning to academia. We have three tips to share with you from our own experiences about how to make the most out of your time at UCL.
Research opportunities
It is absolutely possible to find research opportunities outside of your degree programme. There are multiple health related institutes at UCL including the Institute of Global Health, Institute of Applied Health Research and the Institute of Epidemiology and Healthcare. From our experience, the best way to find research to get involved in is to reach out to academics that work in areas that interest you. Academics frequently have research that Master’s students can volunteer to participate in which isn’t advertised – the only way to find out is to get in contact.
Given the relevance of our Masters, we were both really keen to get involved in research on COVID-19 at UCL. Through reaching out to academics we became aware of new research being run by RREAL and were delighted to be given the opportunity to get involved. RREAL is the Rapid Research Evaluation and Appraisal Lab with international networks co-directed by Cecilia Vindrola-Padros and Ginger Johnson at UCL. RREAL aim to produce relevant and rapid qualitative health research in time-sensitive contexts. We have both joined the RREAL team in conducting their research relevant to COVID-19. This has involved a rapid appraisal of healthcare workers’ perceptions and experiences of responding to the COVID-19 pandemic through analysis of the relevant media, social media, policies and using interviews with healthcare workers. We have been involved in research relevant to the UK, although the study is also being mirrored internationally in 18 countries (at the time of writing). Emerging findings from this research will be published shortly – make sure to look out for this as it will be both of our first publications! Some of the teams’ future publications will consider the impact of the delay or cancellation of elective surgeries, the mental health of healthcare workers and the impact of working in palliative care in the UK during the pandemic. Alongside our UK research, we have both been involved in an opinion piece on the potential impact of COVID-19 in lower- middle- income countries. This paper will be published soon – it makes recommendations based on learning from previous experiences to minimise the impact of this pandemic on fragile healthcare systems. Despite supporting different streams of data collection and analysis, we have both gained valuable skills in conducting qualitative research. We are both really glad that we reached out to find these opportunities and would really encourage others to do the same – you won’t know what’s out there unless you give it a go!
Extra-curricular activities
In order to build on what you learn in your Masters, UCL provides many opportunities to attend events, join societies and go to conferences and free talks from different departments. There are a number of different societies at UCL related to health which include the “Students for Global Health Society”, the “MedTech Society”, the “Application of Psychedelics Society”, “Student Action against Homelessness Society”, “Friends of Médecins Sans Frontières” amongst many others. These societies offer events with opportunities to network with experts and like-minded peers, as well as interesting lectures and stimulating debates. It is very possible to attend events at UCL around your studies, as they are often scheduled at lunch time and in the evenings. In fact, UCL has been running a series called “Lunch hour lectures” since 1942, these lectures are open to everyone for free! These have continued virtually throughout the pandemic and have been really great as a mid-day break from dissertation writing. For example we have recently attended two lunchtime talks called “Trump 2020 and America in a post-COVID world” which was by a lecturer in Global Politics and “Insights from the COVID-19 crisis: useful for the UK’s energy transition to net zero” which was by a Research Fellow at the Energy Institute, BSEER. We would really recommend attending talks and events as they broaden your knowledge beyond module content. They can also be useful for identifying your specific interests which is important for deciding optional modules, dissertation topics and even future careers.
Networking
One huge benefit to seeking research opportunities whilst at UCL and also in attending extra-curricular talks and events is networking. Through attending talks we have been able to meet experts in the field which has been really useful for us to be able to ask career specific questions. Also, through the research that we have been undertaking at RREAL, we have made global connections and built relationships with students from different institutes, public health consultants, and academics from both UCL and other internationally renowned institutions. Networking can be really useful and getting to know people within the different institutes can help with finding a dissertation topic/supervisor and learning about different career paths. If you do this early on you may even find a unique dissertation opportunity that interests you. This is what Kirsi did, she was keen to learn more about digital health interventions so reached out and was able to find a dissertation within a different institute titled “Assessing inequalities in access to STI self-sampling kits across the UK”. Although it may not feel like “networking”, the connections that you make with your peers are also invaluable. We have found that people on our course come from really diverse backgrounds and are at different stages in their careers. This makes for fascinating discussions in lectures and seminars because people can provide insights from their previous experiences working in different countries.
We hope these tips are useful and give you some ideas of extra-curricular opportunities that can work around and compliment your degree programme to help you make the most out of your time at UCL!
Inclusion health and COVID-19
By e.schaessens, on 13 May 2020
Authors: Chantal Edge, Al Story, Andrew Hayward
As the UK continues to wage war against COVID-19 the news is awash with stories speculating when vaccines and diagnostics will become available, and when life can return to ‘normal’ for the general population. Yet amongst these reports we hear very little about society’s most marginalised groups. What has the UK been doing to protect and support the most vulnerable – homeless, prisoners, drug users, and what problems do they foresee for these groups in the near future? We asked the UCL Collaborative Centre for Inclusion Health (CCIH) what they’ve been up to in support of pandemic response.
What is the UCL Collaborative Centre for Inclusion Health?
The UCL Collaborative Centre for Inclusion Health (CCIH) was set up by a multidisciplinary team of researchers, experts with lived experience and frontline professionals who are dedicated to reducing health inequity amongst socially excluded groups. Inclusion Health is a service, research, and policy agenda that aims to prevent and redress health and social inequities among the most vulnerable and excluded populations such as homeless, prisoners and drug users. The Centre is co-directed by UCL’s Professor Andrew Hayward and Dr Alistair Story, Clinical lead of the London Find&Treat Service.
COVID-19 and socially excluded groups
Homeless accommodation
 At CCIH we were very aware early on in the outbreak that excluded groups would be highly vulnerable. There was a well-timed conference – 2020: A Decade for Inclusion – on homeless and inclusion health justbefore the UK went into lockdown, which we used to raise awareness across the homeless sector about what needed to be done to prevent outbreaks, particularly within overcrowded hostels, night shelters and day centres. We were able to secure a lot of support from different agencies, for example, the Ministry of Housing, Communities and Local Government set up an initiative to place those living on the streets in hotels and to close down the large hostels in which people share dormitory-style accommodation. This was achieved incredibly rapidly, over the course of about a week. We’ve also done a lot of work to raise awareness in settings which remain vulnerable to outbreaks, including improving social distancing by encouraging closure of communal areas, and strict rules about social distancing measures. We’ve been able to bring in drug treatment services and addiction services for people with very challenging addiction issues. A pan-London methadone-prescribing service has been established so that homeless people can get access to substitution treatment for addictions much more easily than they would have done on the streets. This video tells the story about one such homeless hotel in Shrewsbury.
At CCIH we were very aware early on in the outbreak that excluded groups would be highly vulnerable. There was a well-timed conference – 2020: A Decade for Inclusion – on homeless and inclusion health justbefore the UK went into lockdown, which we used to raise awareness across the homeless sector about what needed to be done to prevent outbreaks, particularly within overcrowded hostels, night shelters and day centres. We were able to secure a lot of support from different agencies, for example, the Ministry of Housing, Communities and Local Government set up an initiative to place those living on the streets in hotels and to close down the large hostels in which people share dormitory-style accommodation. This was achieved incredibly rapidly, over the course of about a week. We’ve also done a lot of work to raise awareness in settings which remain vulnerable to outbreaks, including improving social distancing by encouraging closure of communal areas, and strict rules about social distancing measures. We’ve been able to bring in drug treatment services and addiction services for people with very challenging addiction issues. A pan-London methadone-prescribing service has been established so that homeless people can get access to substitution treatment for addictions much more easily than they would have done on the streets. This video tells the story about one such homeless hotel in Shrewsbury.
We’ve also established what we’re calling a COVID-CARE hotel in East London for homeless people who are diagnosed as having the disease. They are referred from the streets, hotels, hostels, Secondary Care and A&E departments across the capital to be clinically monitored in a safe infection control environment. The accommodation is provided by GLA, while the medical staff are provided by the UCLH Find&Treat team working with Médicins Sans Frontières (MSF) – this is the first time MSF have deployed in the UK, a video about this work can be found here.
Another aspect of our work has been to establish a surveillance system with UCLH Find & Treat and led by Miriam Bullock, through which we survey hostels for COVID-19 control and social distancing measures, suspected COVID-19 cases and related hospitalisations or deaths. This surveillance system triggers telephone triage and advice from the Find&Treat team who are outreaching same day testing to homeless people across the city with three outreach teams.
Prisons
Public Health England and the prison service have published guidance on their management strategies for COVID-19 in prisons and have as yet managed to avoid the ‘explosive outbreaks’ predicted at the start of the pandemic. Yet healthcare delivery in prisons remains challenging now that inmates are confined to their cells for up to 23 hours a day and many staff are off sick or isolating with COVID-19 symptoms.
One of the CCIH PhD fellows, Chantal Edge, has paused her work on local prison telemedicine implementation in Surrey, to go to the central NHS England Health and Justice team to lead on the rapid deployment of prison telemedicine nationally. Telemedicine will be scaled up across 135 secure sites in England including prisons, immigration removal centres and secure children’s homes. Approvals have also been secured from the prison service to deploy NHS 4G enabled tablets in prisons to support the telemedicine work, a ground-breaking change seeing as mobile devices are traditionally strictly prohibited in prison settings. Telemedicine will remain in prisons after the pandemic and support improved access and quality of healthcare services for prisoners, so in this way the pandemic has driven forward innovation.

Migrant health
Ines Campos Matos, who has a joint appointment between PHE and CCIH has led PHE’s investigation of the high levels of COVID in BAME groups showing how poverty is compounding this inequality.
Advocacy in the media
We have also been working closely with the press to advocate for inclusion health groups including articles on prisons, and homeless hotels and GP surgeries.
Looking to the future
As COVID-19 decreases in the general population following lockdown, we’re moving to a stage of continued vigilance. This is going to be really important because there are likely to be more transmissions when the lockdown is eased. So far, we have avoided large outbreaks of COVID-19 in the homeless community and in prisons. In other countries such as the USA up to half of people in big, night-shelter-type hostels are being infected, our screening finds only about 3 or 4% of homeless people have been infected. Prisons in countries such as Italy and the USA have also seen huge outbreaks, whereas cases in England remain controlled.
There is a concern that people will begin to think the outbreak is over and will start to relax both the social distancing across society but also in the homeless hostels. As the numbers decrease, there will be pressure to close down the COVID-CARE facility and the hotels. Prisons will likely need to keep measures in place to isolate the vulnerable and enforce social distancing for many months, the mental health consequences of this enforced isolation remain as yet unknown.
We’re planning to launch a major health needs assessment (HNA) led by Dr Binta Sultan, to systematically identify the health needs of people within the hotels. We’ll have 38 clinicians doing telephone interviews, and have established referral pathways into mental health, sexual health and drug and alcohol services. We’ll be screening everybody for hepatitis C, then starting people on treatment with the aim of completion while they’re at the hotel. This could have a major impact on the transmission of hepatitis C in the homeless population. We’re hoping to do the same thing for latent TB infection. The HNA will also identify people who need shielding, therefore requiring their own self-contained accommodation. This will move people up the priority list for permanent housing and will help with advocating for their needs.
During this pandemic, many of us are having to change what we do and prioritise everything towards this response. It’s too serious and awful to feel any excitement about the research: it feels more like a war. We’re trying to use every resource and opportunity that we have – and every waking hour – to work out what we can do to help in the fight against COVID-19. It is rewarding to feel that you’re able to make a difference, but it’s heart-breaking to see how terrible it has become.
Chantal Edge is an NIHR Clinical Doctoral Research Fellow and Specialty Registrar in Public Health, researching the use of telemedicine for hospital appointments in prison. Dr Al Story leads the Find&Treat Outreach Service based at UCLH and is Co-Director of the UCL Collaborative Centre for Inclusion Health. Professor Andrew Hayward is the Director of the UCL Institute of Epidemiology and Health Care and Co-Director of the UCL Collaborative Centre for Inclusion Health.
The benefits of a clinic visit: How I connected course learning, personal experience and observing a professional
By e.schaessens, on 24 April 2020
by Katie Gilchrist
I am an MSc Health Psychology student at UCL. As part of the programme, we are required to attend a clinic for observation. As a brain tumour survivor, a natural choice for me was the Neurosurgery clinic at The Unit of Functional Neurosurgery at The National Hospital for Neurology and Neurosurgery, London.
My sense of tumour

In December 2017 I was diagnosed with a benign brain tumour called acoustic neuroma and in February 2019 I underwent surgery at The Royal Randwick hospital in Sydney, Australia to have the tumour removed. A consequence of the surgery was being left with grade 6 House-Brackman facial paralysis, single sided deafness and one less vestibular nerve. I spent the first month recuperating from the surgery, practicing walking with one balance nerve and adjusting to losing the hearing in one ear and the loss of facial movement on one side of my face. Seven months after the surgery my husband and I packed up our lives after spending seven years in Australia and moved back to the UK where I started my MSc in Health Psychology at UCL. Following my experience, naturally, I was really excited about spending a morning in a hospital clinic (a mandatory part of the course) and even more excited when I saw there was a neuro clinic!
Feeling empathy for patients
So, recently I attended the clinic at The Unit of Functional Neurosurgery at The National Hospital for Neurology and Neurosurgery, London with Prof Ludvic Zrinzo. The clinic specialises in cranial nerve disorders such as hemifacial spasm (involuntary facial twitch) and trigeminal neuralgia (chronic facial pain). What I didn’t realise, when I made my selection, was that the conditions Prof Ludvic Zrinzo works with can present with facial droop or weakness and that for some of the conditions the surgical approach, risks and recovery are very similar to what I had. There were a lot of patients with facial movement issues and their faces looked like mine, asymmetrical smiles and one eye looking frozen open, foreheads not able to move and I felt such empathy for them. It was difficult not to run after them and comfort them but at the same time it was like hearing my own diagnosis over and over again. There were several moments where my eye (only one produces tears) glazed over and I had to concentrate not to show too much emotion as that would have been unprofessional. While it may help the patient to see we are human, it is not good for them to feel our burden which may accidentally transfer to them if we overshare.
 Learning from the best
Learning from the best

Having met a few surgeons through my own health experience, I was really blown away by Prof Ludvic Zrinzo’s approach to patient care. It was great to see a surgeon putting into practice all the psychology aspects we have learned in class this term; building rapport, explaining in clear language, allowing time for the patient to ask questions as well as all the additional points he covered like asking who was at home to help with care, reminding them to bring partners into appointments and explaining all the options available to them and really emphasising that it was the patients decision. Before each consultation, he explained to the patient who we were (there were three students observing) and he asked if it was ok if we stayed and listened. Only one patient decided at that time it was not ok for us to stay for that appointment and Prof Zrinzo kindly asked us to wait outside. On our return we didn’t ask about the patient and nor did he offer any information. The appointment had taken longer than some and we were playing catch up. I also felt there was an understanding between us that in this instance any discussion was to stay between patient and health professional.
What will I take from this into my future roles?
- The importance of asking the patient what they want
- Did they mind having students in the room?
- What were their thoughts on which treatment?
- The benefits of open dialog
- Encouraging patients to include family and friends in the conversation
- Explaining risks and benefits in layman’s terms without provoking fear
- Asking about family, other health issues, home/work environment
- Having open discussion with empathy and patience, even if it has been discussed several times previously
Overall, Prof Ludvic Zrinzo had such a great approach and I am so grateful to be able to have observed this. While it was emotional for me it really reaffirmed my desire to help people with health issues and I just wanted to say thank you to UCL and The National Hospital for Neurology and Neurosurgery for arranging such a great experience.
Being out at work
By e.schaessens, on 24 April 2020
An interview with Dr Julia Bailey by Sandra Medina and Angela Gichane (before the Covid-19 crisis)
Thank you for doing this interview with us. Can you tell us about your job?
I am a sexual health doctor in South East London, and senior researcher in the eHealth Unit at UCL. I teach medical students, NHS staff and researchers, and am also a Graduate tutor and co-chair of the Equality Action Group.
What is your experience of being out at work?
I came out in 1987, when I was a medical student – 33 years ago! I’ve always been open about my sexuality (lesbian), but it doesn’t feel particularly relevant at work. I’ve never felt that that my sexuality was an issue working in primary care and in sexual health: these specialities tend to attract open-minded people, and I know of quite a few LGBQ (lesbian, gay, bisexual, queer) colleagues. Trans and Intersex people are less visible in academia and the NHS – we have a lot further to go in helping trans and intersex people feel seen, safe, welcome and included.
I haven’t experienced overt discrimination at work, but my sexuality has shaped (and limited) my choices. For example, I live in London to be part of the queer community, rather than risk feeling alienated in a small, conservative community.
Is visibility important?
A very important role model for me in my teens was the conductor of the Brighton Youth Orchestra (David Gray), who was a fantastically inspiring musician who was gay. His sexuality was well known, and there was no fuss about it (40 years ago).
At medical school there weren’t any visibly out members of staff, and no out students either – I found my community outside the medical school. I bumped into someone years later who told me that I had been an important role model for her at medical school, which was lovely to hear. As Dr Ronx (the queer, Black, androgynous A&E doctor) says, ‘You cannot be what you do not see’, and I think being visibly out is important.
How can tutors can support LGBTQIA* students?
It is really important that students can trust tutors, and that students feel able to talk about life beyond their studies (if they want to). I don’t proactively ask students about their personal lives, but I do tell them that I’m happy to discuss anything that affects their learning or wellbeing.
* LGBTQIA – lesbian, gay, bisexual, trans, queer, intersex, asexual/aromantic
Many people are quite confused about gender, sexuality, pronouns…. can you give us a summary?
Ah yes – I’ve written an e-learning module on this, and I train GP registrars and sexual health clinic staff. There is a lot of confusion, and concepts and language are changing over time …
Gender
In most societies worldwide people are seen as either ‘male’ or ‘female’ (i.e. binary categories). These categories are decided (assigned) at birth, usually on the basis of genital appearance. A proportion of the population are intersex – i.e. their genetics, genitals and/or hormones are more complex than neat binary ‘male’ or ‘female’ categories.
Whilst sex and sex variation (male, female, intersex) are defined by genetics, gender identity is someone’s internal sense of gender (e.g. masculine, feminine, intersex, non-binary). Gender expression is the way that gender is expressed to others (e.g. through clothes, the body, behaviour…). Cis gender means that a person’s gender identity is the same as the gender they were assigned at birth (e.g. someone who was assumed to be female at birth, and who identifies as a woman). The terms Assigned Male at Birth (AMAB) and Assigned Female at Birth (AFAB) acknowledge someone’s gender history.
Non-binary or genderqueer people are those whose gender identity does not align with either ‘male’ or ‘female’, and who do not subscribe to conventional gender distinctions. Non-binary and genderqueer identities may be static or fluid. Some people may include aspects of ‘male’ and ‘female’ into their identities, others may reject binary gender categories entirely. Non-binary and genderqueer people may or may not look androgynous (not looking typically masculine or feminine).
Transgender or trans is a term for people who have a gender identity or gender expression that differs from their assigned gender. For example this could be someone who was assumed to be female at birth whose gender identity is male.
Pronouns (such as he, she, they) are very important in affirming someone’s gender identity.
Non-binary people may choose the pronoun ‘they’ as a gender neutral pronoun which is neither male nor female. There are other gender neutral pronouns (e.g. ze, sie, hir, co, per, ey), and terminology concerning gender identity is evolving. It is important not to just guess or assume someone’s gender identity and pronouns.
Gender is distinct from sexuality. For example, ‘gay’, ‘lesbian’ or ‘bisexual’ are sexualities (sexual orientations), i.e. expressions of sexual attraction. Gay men are typically attracted to male sexual partners; lesbians to female sexual partners; bisexual people are attracted to people of the same or different genders to them. LGBTQIA stands for Lesbian, Gay, Bisexual, Transgender, Queer, Intersex and Asexual/Aromantic. There are many, many other ways of expressing sexuality.
What would help trans and non-binary people feel welcome and included?
Getting people’s gender correct is really important, and it makes a huge difference to be asked rather than just guessing gender and pronouns (he, she, they) from someone’s appearance. This is especially important for trans and non-binary people, for whom mis-gendering can be relentless and horribly undermining.
My pronoun is ‘she’, but I also feel non-binary/genderqueer – I find it liberating to move away from the assumptions and expectations that go with being either male or female. It grates to be identified as a lady: e.g. “Good evening ladies and gentlemen…”. ‘Lady’ does not describe me, and it feels irrelevant and distracting – what does my gender have to do with being in a lecture, meeting, restaurant etc.? I feel that the assumptions and expectations of ‘men’ and ‘women’ can be profoundly harmful and limiting, and we should all be free to express ourselves however we like. 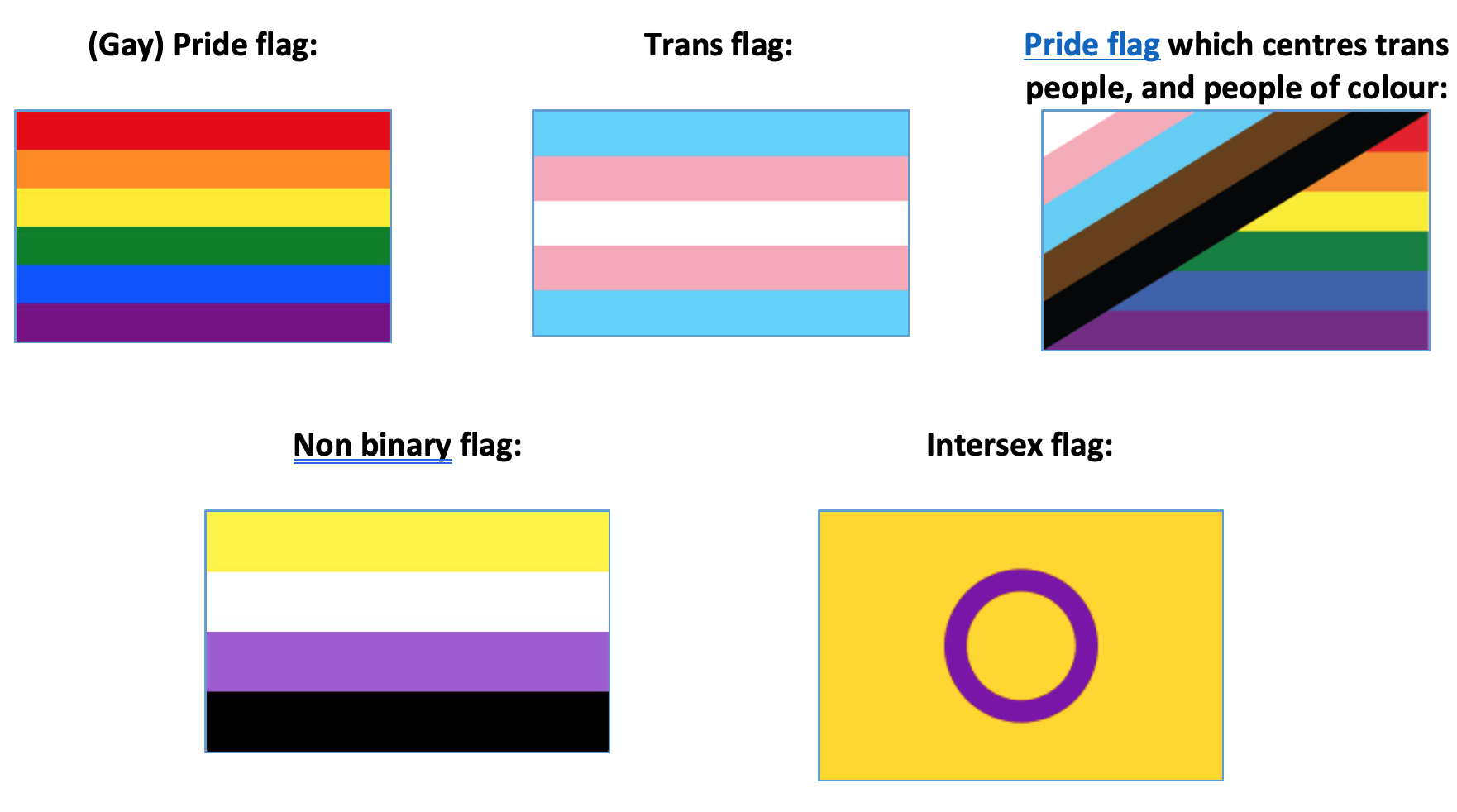 We’re a long way from that vision, and expression can be especially hard for people who are marginalised in more than one way (e.g. trans women of colour). We have a lot of work to do to ensure that trans, non-binary and intersex people feel safe to be themselves at work.
We’re a long way from that vision, and expression can be especially hard for people who are marginalised in more than one way (e.g. trans women of colour). We have a lot of work to do to ensure that trans, non-binary and intersex people feel safe to be themselves at work.
As tutors and colleagues, we can demonstrate inclusive attitudes to gender and sexuality by displaying LGB, trans, non-binary and intersex stickers, badges or lanyards, and including logos and our own pronouns in email signatures for example.
For email footers:
Out@UCL logo which acknowledges people of colour and trans people:

How can we create a more inclusive workplace?
I think that social events are a good idea, to help people get to know each other. We need to check whether there barriers to being involved:
- Equality. can everyone afford to come?
- Diversity: is the invitation genuinely open to everyone?
- Inclusion: are there factors that will exclude some people, such as alcohol, caring responsibilities, noise levels, access…..
‘Core competence’ in gender and sexuality is important, so that all staff are familiar with issues that LGBTQIA staff and stu dents may face. It’s important to avoid assumptions, and check people’s preferences in terms of gender, pronouns, and confidentiality for example.
dents may face. It’s important to avoid assumptions, and check people’s preferences in terms of gender, pronouns, and confidentiality for example.
We need to avoid assuming heterosexuality, and avoid the gender binary – for example, ask say “Good afternoon everyone” instead of ‘Good afternoon ladies and gentlemen’. You can’t guess someone’s gender or sexuality by appearance, and there are far more LGBTQIA people than widely assumed.
Thank you, do you have anything more to add?
Thank you Angela and Sandra, it has been really interesting talking to you. It has reminded me how important these issues are!
Sources of support for LGBTQIA staff and students
Time to help our children get a move on
By guest blogger, on 17 January 2020
World Health Organisation and United States guidelines say adolescents should do at least an hour’s moderate-to-vigorous physical activity each day. But a new global study shows eight out of 10 fail to meet that standard – and there is a widening gender gap. Professor Yvonne Kelly and Fran Abrams outline new research revealing worrying trends which demonstrate the need for political and social choices that will help young people enjoy the social, physical and mental benefits of being active.
Physical activity has many health benefits for young people – and globally, four in every five adolescents do not benefit from regular physical activity.
In 2018, the WHO launched a global action plan called More Active People for a Healthier World. It aimed to reduce the proportion of people doing insufficient physical activity by 15 per cent by 2030 among both adolescents and adults.
Now in a major new study WHO researchers have analysed information on 1.6 million school students aged 11-17 in 146 countries. They found some positive trends but argued much still needed to be done to encourage young people to exercise more.
There was a small reduction over 15 years in the proportion of boys not doing enough, though this still fell well short of the WHO’s target. But the proportion of girls meeting the target remained static and this led to a widening gender gap.
As has been shown in the UK such gender differences start early with lower levels of physical activity in girls emerging before they become teenagers.
The authors of a separate investigation using the Millennium Cohort Study (MCS) suggest the main reason for young people not exercising or sleeping enough is the amount of time they spend using screens. This is a hotly contested area, intuitively, ‘too much screen time’ and ‘too little exercise’ might appear to sit side by side. However, in this kind of study, it is not possible to infer that one causes the other.
The WHO study showed the majority of adolescents did not meet physical activity guidelines, putting their current and future health at risk. Although there were small reductions in insufficient activity among boys, the prevalence of insufficient physical activity in girls had remained unchanged since 2001.

Figure 1 Prevalence of insufficient physical activity among school-going adolescents aged 11–17 years, globally and by World Bank income group, 2001 and 2016
Huge dataset
The dataset used in the WHO study was huge – the young people studied had provided information for at least three years and the analysis covered four World Bank income groups, nine regions, and the globe as a whole for the years 2001–16. Saying that, although the research data covered more than 80 per cent of the global population, it still didn’t cover every county and region. And the estimates for low-income countries need to be treated with caution as the coverage there was much lower – only 36 per cent.
The overall analysis showed that more than eight out of 10 school-going adolescents aged 11–17 did not meet the recommendations for daily physical activity. The small improvements in boys’ activity levels, combined with the static position in girls’ activity, suggested a target of more than 30 per cent of adolescents meeting the recommended level by 2030 will not be met.
Globally, across all income groups and regions and in nearly all the countries analysed, girls were less active than boys.
And perhaps surprisingly, the research did not find that the problem was worse in higher-income countries. However, this was not the case for girls, for whom there was no clear pattern in relation to country income.
Differences in activity levels
In addition to variations related to gender and affluence, there were also differences in activity levels between different parts of the world. The boys least likely to meet activity targets were in the high-income Asia Pacific region, but the second-least likely were in lower-income Sub-Saharan Africa and particularly in Sudan and Zambia.
The boys most likely to meet the targets were found in high-income western and south Asian countries with large populations such as the USA, Bangladesh, and India.
These variations might be driven by specific characteristics of particular countries – for example, as the research looked at school children the picture might be skewed in countries where disadvantaged children often do not attend school, or in places where the tradition of school or community sport is strong.
For girls, the largest proportions failing to meet the targets were in Asia Pacific and particularly in South Korea- though in some of those countries girls’ participation in education is low and that might have affected the study’s sample.
The recent MCS study by academics from Loughborough University and University College London used data from 3899 adolescents. This study, in which young people were fitted with activity monitors, found that while nine out of 10 were getting the recommended amount of sleep, just four in ten met exercise targets and a quarter were keeping to the recommended screen time. These figures were higher than those in the WHO study, which could be explained by the different methods used to measure activity and which show just how important it is to consider HOW activity is measured.
The study looked at some correlates of physical activity and showed that adolescent girls who had depressive symptoms were less likely to meet all three of these recommendations (8-10 hours of sleep, no more than two hours of screen time and at least an hour a day of physical activity), while those from better-off backgrounds were more likely to meet them. Among boys, those who were obese and those who had depressive symptoms were less likely to meet the recommendations. However, it is not possible to rule out the potential for cyclical associations to be at play here as low levels of physical activity could lead to depressed mood and to weight gain.
What can be done?
- More research is needed to understand the causes of non-participation in exercise – social, economic, cultural, environmental and technological.
- Policy change should be prioritised and should encourage all forms of physical education – sport, active play, and recreation as well as safe walking and cycling.
- Social marketing campaigns such as the National Lottery funded #thisgirlcan campaign combined with community-based interventions could be starting points to increase physical activity levels in girls, particularly in countries with wide gender differences. This approach has been identified as cost-effective.
- Schools, families, sport and recreation providers, urban planners, and city and community leaders all need to become involved.
That four in every five adolescents do not experience the enjoyment and social, physical, and mental health benefits of regular physical activity is not a chance thing – it is the consequence of political choices.
Young people have the right to play and should be provided with the opportunities to realise their right to physical and mental health and wellbeing. Urgent action is needed, particularly through targeted interventions to promote and retain girls’ participation in physical activity. Policymakers and stakeholders should be encouraged to act now for the health of this young generation and of future ones.
Yvonne Kelly is Professor of Lifecourse Epidemiology and Director of the ESRC International Centre for Lifecourse Studies at UCL. She is editor of the Child of our Time blog.
Fran Abrams is CEO of the Education Media Centre and freelance journalist who writes for the Child of our Time blog.
Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants, by Regina Guthold, Leanne Riley, Fiona Bull and Gretchen Stevens, is published in The Lancet Child and Adolescent Health.
Regina Guthold, Leanne Riley and Fiona Bull are based at the Department for Prevention of Noncommunicable Diseases, WHO, Geneva, Switzerland and Gretchen Stevens is at the Department for Information, Evidence and Research, WHO, Geneva, Switzerland. Fiona Bull is also affiliated with the Department of Sport and Exercise Science, University of Western Australia, Perth.
Prevalence and Correlates of Meeting Sleep, Screen-Time, and Physical Activity Guidelines Among Adolescents in the United Kingdom, by Natalie Pearson, Lauren B Sherar and Mark Hamer, is published in JAMA Paediatrics:
Natalie Pearson and Lauren Sherar are at the School of Sport, Exercise & Health Sciences, Loughborough University, United Kingdom, and Mark Hamer is at the Institute of Sport Exercise & Health, Division of Surgery & Interventional Science, Faculty of Medical Sciences, University College London, United Kingdom.
This blog article is courtesy of the Child of our Time blog, which is a blog about the health and happiness of children living in the UK. led by the ESRC International Centre for Lifecourse Studies, University College London
Are some types of job bad for your mental health?
By guest blogger, on 17 January 2020
 Mental illness is a major cause of early retirement – but do those who are forced to leave work early for this reason get better afterwards? What is the relationship between work stress and mental health? A new study of public sector workers in Finland suggests there is a link – and there are important lessons for employers. Tarani Chandola from the ESRC International Centre for Lifecourse Studies was among the authors of the study.
Mental illness is a major cause of early retirement – but do those who are forced to leave work early for this reason get better afterwards? What is the relationship between work stress and mental health? A new study of public sector workers in Finland suggests there is a link – and there are important lessons for employers. Tarani Chandola from the ESRC International Centre for Lifecourse Studies was among the authors of the study.

One way in which we can track the prevalence and level of mental illness is by looking at the use of psychotropic medication – that is, medication which can alter one’s mental state. This group of drugs includes common antidepressants, anti-anxiety drugs and antipsychotic medication.
If there is a link between work stress and mental illness, then we should expect those forced to leave work for this reason to get better after retirement. So by tracking the levels of psychotropic medication among a group of workers before and after retirement, we could find out the extent to which there was such a link.
We were able to use data from a long-term study of Finnish public sector workers to examine the issue more closely.
It matters because previous studies have shown an increase in the use of this group of drugs among all those who take disability retirement, particularly those whose retirement was due to mental ill health. Those from higher social classes saw the biggest drop in medication use after retirement, suggesting there are social factors at play here, too.
Global issues
The effect does seem to vary around the globe, though – some studies from Asia found an increase, rather than a decrease, in mental health problems after leaving work. But in Europe, retirement has often been found to be followed by an improvement in both mental and physical health. Retirees have reported sleeping better, feeling less tired and generally feeling a greater sense of wellbeing.
We were able to use data from the Finnish Public Sector study cohort study, which followed all employees working in one of 10 towns and six hospital districts between 1991 and 2005. The study included participants from a wide range of occupations including administrative staff, cleaners, cleaners and doctors, and they were followed up at four-year intervals regardless of whether they were still in the same jobs. Their survey responses were linked to a register of medication purchases for at least two years before retirement and two years after.
We had information on 2,766 participants who took retirement because of disability. Uniquely, the data included both participants’ use of medication and their perceived levels of work stress. So we were able to ask whether there were differences in this pre and post-retirement effect between those in low and high-stress jobs.
Specifically, we looked at something called effort-reward imbalance – that is, when workers put in too much effort at work but get few rewards in compensation: according to a recent review, this carries an increased risk of depressive illness.
If our theories were correct, we would see a decline in the use of psychotropic medication after disability retirement, and it would be greatest among those with high levels of effort-reward imbalance. Along with mental illness the other major cause of disability retirement in Finland is musculoskeletal disease, so we categorised our sample in three groups – mental illness, musculoskeletal disease and ‘other.’ Eight out of 10 in the sample were women, and three out of 10 reported high effort-reward imbalance before retirement.
Unsurprisingly, those who retired due to a mental disorder had the greatest increase in psychotropic drug use before retirement. And those who were in high-stress, low-reward jobs had higher levels of medication use than those who were not. But after retirement, there was no difference in psychotropic drug use between those with high vs low effort-reward imbalance. It looked as though stopping work in high stress jobs reduced the need for higher psychotropic medication use among those workers who exited the labour market for mental health reasons.
Retirement because of musculoskeletal disease or other causes was not associated with any similar link between stress level and psychotropic medication.
Lessons for employers
Our study showed that among people retiring due to mental disorders, those in high-stress, low-reward jobs benefited most from retirement. So it’s likely that they could benefit from the alleviation of work-related stress before retirement, too.
In conclusion, if employers could find ways of reducing the levels of stress suffered by employees suffering from mental ill-health, their early exit from paid employment might be prevented and their working lives might be extended.
Psychotropic medication before and after disability retirement by pre-retirement perceived work-related stress was published in the European Journal of Public Health, Vol. 0, No. 0, 1–6.
The other authors were Jaana Halonen, Taina Leinonen, Ville Aalto, Tuula Oksanen, Mika Kivimäki and Tea Lallukka of the Finnish Institute of Occupational Health; Hugo Westerlund and Marianna Virtanen of the Stress Research Institute, Stockholm University; Martin Hyde of the Centre for Innovative Ageing, Swansea University; Jaana Pentti, Sari Stenholm and Jussi Vahtera of the Department of Public Health, University of Turku; Minna Mänty of the Department of Public Health, University of Helsinki; Mikko Laaksonen of the Research Department, Finnish Center for Pension.
These authors also have the following additional affiliations: Jaana Halonen; Stress Research Institute, Stockholm University; Jaana Pentti; Department of Public Health, University of Turku; Minna Mänty; Statistics and Research, City of Vantaa, Finland; Mika Kivimäki, Department of Public Health, University of Helsinki and Department of Epidemiology and Public Health, University College London; Marianna Virtanen, School of Educational Sciences and Psychology, University of Eastern Finland, Joensuu; Tea Lallukka, Department of Public Health, University of Helsinki.
This blog article is courtesy of the Work Life blog, which is a blog about the relationship between work and health and well-being of people, whether they are preparing for working life, managing their work / life balance or preparing for retirement and life beyond retirement. Led by the ESRC International Centre for Lifecourse Studies, University College London
Tailoring cessation support for disadvantaged smokers – is it working?
By e.schaessens, on 5 December 2019
Author: Loren Kock, PhD student, Tobacco and Alcohol Research Group
 Smoking cigarettes remains a leading cause of preventable death and disease in many high-income countries. Most of these harms fall disproportionately upon socioeconomically disadvantaged individuals who generally have greater difficulty in quitting and remaining abstinent. In increasingly resource constrained health systems, what role does behavioural support that is tailored to an individual’s socioeconomic position (SEP) play in helping smokers quit and stay quit?
Smoking cigarettes remains a leading cause of preventable death and disease in many high-income countries. Most of these harms fall disproportionately upon socioeconomically disadvantaged individuals who generally have greater difficulty in quitting and remaining abstinent. In increasingly resource constrained health systems, what role does behavioural support that is tailored to an individual’s socioeconomic position (SEP) play in helping smokers quit and stay quit?
Reducing health inequalities, which includes access and provision of health-care services, has been included as one of the UN’s sustainable development goals (SDG 10). Given that smoking is estimated to kill almost 8 million people a year and largely falls along a socioeconomic gradient, acting to prevent uptake of smoking and to help existing smokers quit is an essential part of this goal. Alongside other interventions and policies, the WHO’s ‘MPOWER’ package of measures to reduce the prevalence of smoking worldwide, provision of behavioural support to individuals trying to quit smoking is widely thought to be an effective approach. An advantage of these interventions is that health providers can be flexible in their delivery; support can be delivered in-person or over the phone, via digital media or through the use of financial incentives.
To tailor or not to tailor?
Even with the best support, most people relapse to smoking within the first month of quitting. Interventions that are tailored to smokers from disadvantaged groups stem from the knowledge that these individuals have greater difficulty in quitting and remaining abstinent than do those from more affluent groups. This is largely due to issues such as financial stress, absence of social support, addiction, lower confidence, stress, scarce life opportunities and less interest in the harms related to smoking. Because they don’t specifically address these barriers, it is generally thought non-tailored interventions are generally less effective among disadvantaged groups and may therefore be exacerbating existing inequalities. Compared with interventions that have no specific demographic target (non-tailored), interventions that are tailored to address these socioeconomic barriers (SEP-tailored) could, at least in theory, be more successful.
Our study published in the Lancet Public Health sought to tease out how much more effective, if at all, SEP-tailoring was for helping socioeconomically disadvantaged smokers quit.
Is SEP-tailoring more effective?
Our analysis of long-term (6 month) smoking cessation among disadvantaged participants from 42 randomised controlled trials revealed that individual-level behavioural support, regardless of whether or not it is tailored, can assist disadvantaged smokers with quitting. As aforementioned, tailored approaches specifically are expected to have an important role in reducing health inequalities by addressing some of the needs specific to disadvantaged smokers. However, further analysis revealed that when compared with not tailoring, SEP-tailoring was no more effective.
Quitting is hard
These results highlight the challenges that disadvantaged smokers face when making a quit attempt. It’s likely that behavioural support is effective in the short term, but the benefits wear off or disappear entirely when weighed against the circumstances and stresses that a recently quit ex-smoker faces every day. Dealing with the cravings and withdrawals associated with abruptly coming off the highly dependence-inducing nicotine from cigarettes, while also having to face unstable employment, low income, poorer housing conditions and general lack of support makes it much more likely that a disadvantaged ex-smoker will find themselves returning to smoking. It may be that even when tailored behavioural support attempts to adjust for SEP, it isn’t quite enough when weighed against these life circumstances. However, although no more effective than non-tailored approaches, tailoring is still an effective method; our analysis estimated that all types of behavioural support can improve quit rates by over 50%.
Doing more, and better
These findings don’t imply that tailored approaches should be abandoned. Instead, they should be a call to action for improved, multifaceted approaches at the individual, community, and population level that recognise the wider context of socioeconomically disadvantaged smokers. Sometimes complex problems require complex solutions!
Read the paper: https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(19)30220-8/fulltext
Taking the me out of social media
By guest blogger, on 9 October 2019
 Emma Walker, second year BBSRC-ESRC funded Centre for Doctoral Training in Biosocial Research PhD student at University College London’s Institute for Epidemiology and Health Care, describes how getting involved with research on social media helped her to reflect on her own usage.
Emma Walker, second year BBSRC-ESRC funded Centre for Doctoral Training in Biosocial Research PhD student at University College London’s Institute for Epidemiology and Health Care, describes how getting involved with research on social media helped her to reflect on her own usage.
It’s 00.23 and I should be in bed. I’ve got lots on tomorrow but I’ve spent the last 45 minutes scrolling. Scrolling through the profiles of Instagram “life style coaches”, yogis, models; each collection of photos perfectly curated to appeal to my desire for millennial aesthetic.
Everything feels so much better than anything I have. And actually, in the world of Instagram, I know that everything is much better than what I have. Number of followers or number of likes on each post has conveniently quantified this for me.
The next evening, as part of my public health PhD work, I’m reading Professor Yvonne Kelly’s paper laying out the effects of social media use on the mental health of girls. I diligently make notes “.. greater social media use related to online harassment, poor sleep, low self-esteem and poor body image .. ” “..girls affected more than boys..” and pause periodically to check my phone.
All my friends are at the pub having a great time, another friend just put up a post where she looks amazing, it already has 50 likes. I get to the methods section of the paper “how many times in the last 2 weeks have you felt miserable or unhappy; found it hard to think properly or concentrate; felt lonely; thought you could never be as good as other kids…”.
Then the penny drops. Why do I think I’m immune? I’m like the lifelong smoker who’s confused by their cancer diagnosis: “I never thought it would happen to me.” The idea starts to filter in: I don’t need this in my life. In fact, I need this to not be a part of my life.
The next day I deactivate my Instagram account. That day I meet a friend for coffee in a hipster café and don’t take a picture of my coffee. That night I get to sleep by 11pm. The next day I work more productively than I’ve worked in weeks.
An opportunity to get involved comes up: the National Literacy Trust are really interested in Yvonne’s work and are keen to put together an event for young people. A great group of undergraduates and I devise a series of activities to find out what young people think about the research.
The first section would involve 4 zones at the front of the Renaissance Learning centre room for Strongly Disagree, Disagree, Agree and Strongly Disagree we put a series of statements on the board and ask the pupils to move to a zone and explain why. We include statements on a range of topics including cyber bullying, sleep deprivation, self-esteem and body image and parents and social media.
On the day, the 50 enthusiastic 11-14 year olds from 3 schools across London jostle about, keen to share their opinions and to hear one another’s. I’m amazed at the diversity of ideas, overall willingness to get involved and the mental health literacy of many of the students.
Some responses are predictable; the boys happy to appear less concerned about body image, many keen to state in front of their teachers that social media does not in any way disrupt their studies. Some are surprising; only a handful of pupils had been on social media before arriving at the event that day (a significantly lower proportion than the adults running it!) Other responses are hard to read; were the gaggle of girls laughing at the very idea of social media posts making you feel left out, honest or desperate to seem not to care?
A clear feeling was the young people’s frustration at their parents use of phones and social media. Many expressed irritation at the rules their parents have established – no phones at the table, in bedrooms, after 8pm – that they, themselves constantly break.
One boy described having to ask the same question 3 times before his dad will look up from his phone. The idea that our event should be run for parents was cheered.
Next we presented them with the evidence base for the possible impact of social media and mental health then asked them to make public health campaign like posters with top tips that could go up in their schools. We were presented with a beautiful collection of posters with thoughtful advice, carefully put together information, clever slogans and eye catching drawings. Audio recordings from the day gave further insights from the young who readily offered tips and advice for younger children.
Overall, I think the event was a success. My main impression was that these young people are actually very well equipped to protect themselves from the potential mental health impact of social media. That in fact it may be people in their 20s, who have grown up in the full glare of social media and its pressures, who are at the greatest risk.
It was a real privilege being able to discuss this topic with young people and the message that stood out the most from them is the opportunity parents have to make a difference by practicing what they preach. Chances are they’ll benefit from switching off!
As for me, it’s now been 6 months since I deleted Instagram and whilst it hasn’t been plain sailing – I have got this itch for the buzz of an influx of likes – for the time being I’m happy and I would wholeheartedly recommend it!